Return to Case of the Month Archives
A Single Radiolucent Lesion in the Anterior Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Rick Edwards, Federal Way Oral Surgery
Case Summary and Diagnostic Information

This is a 16-year old white male referred by the orthodontist to the Oral Surgeon to evaluate a single radiolucent lesion in the anterior mandible. It was discovered during routine radiographic evaluation by his orthodontist. The lesion was asymptomatic; there was no swelling or pain.
Diagnostic Information Available
This is a 16-year old white male referred by the orthodontist to the Oral Surgeon to evaluate a single radiolucent lesion in the anterior mandible. It was discovered during routine radiographic evaluation by his orthodontist. The lesion was asymptomatic; there was no swelling or pain.
His past medical history and family history were non-contributory. The patient and his mother did not recall an event that could have led to this lesion, such as history of trauma to the area. The patient was not on any medications.
The clinical examination revealed no evidence of swelling or pain. Radiographic findings were positive for a well-defined and partially corticated 1 X 2 cm unilocular radiolucency at the apex of teeth #s 22-23 (Figure 1). The lamina dura and periodontal ligament of these two teeth were intact and the teeth were vital. The patient also had a developed crown of teeth #s 1 and 16 surrounded by a dental follicle.

Figure 1. Panoramic view at first presentation demonstrating a well-demarcated, round and unilocular radiolucency at the apices of teeth #s 22 and 23. Notice the developed crowns of teeth #s 1 and 16 each surrounded by a dental follicle.
The excisional biopsy revealed small fragments of bone and fibrous connective tissue. Bone comprises the bulk of the specimen, is viable, and is both reparative and lamellar in type (Figure 3). The bony fragments contain spaces filled with loose and vascular fibrous connective tissue (Figure 4). Note that clusters of extravasated erythrocytes are also present .
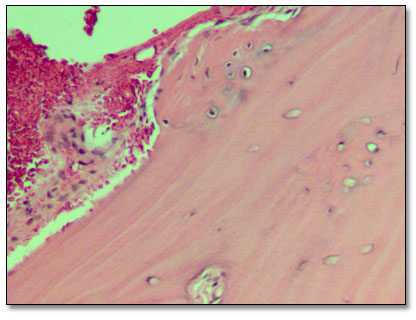
Figure 3. Low power (x100) histology shows small fragments of lamellar bone with viable osteocytes and small fragments of loose and vascular connective tissue within small spaces and around the bony fragments.
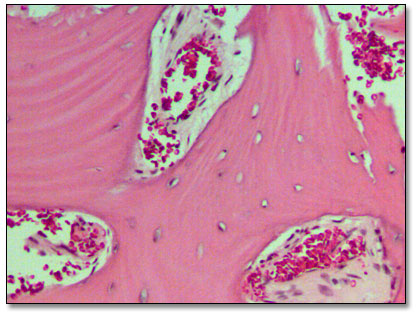
Figure 4. Higher power (x200) histology shows lamellar bone and loose fibrous connective tissue.
After you have finished reviewing the available diagnostic information