Unilocular radiolucency between teeth #s 26 & 27
Can you make the correct diagnosis?
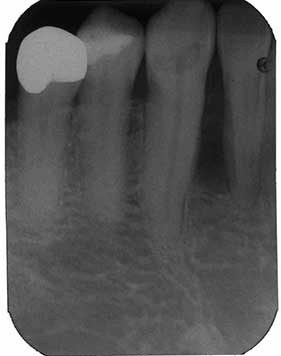
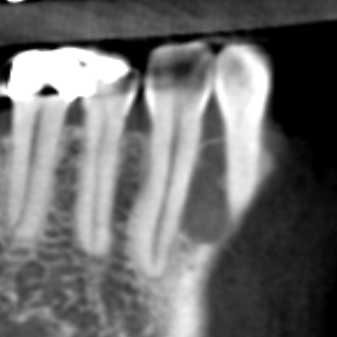
This is a 66-year-old male who presented for diagnosis and treatment of a radiolucent lesion between #s 26-27 (Figures 1-2).
Sorry, you are incorrect!
A well-defined radiolucent lesion between the right mandibular lateral incisor and canine teeth involving the full length of the roots raises the possibility of a botryoid odontogenic cyst (BOC). BOC is more likely in this case than a lateral periodontal cyst, since the latter tends to present more in the upper or middle third of the roots. However, BOC tends to be radiographically multilocular, which this lesion is not. Although the radiographic findings do not support a multilocular lesion, the surgical notes indicate a lesion with multiple compartments that were not appreciated on the radiograph. The patient’s age is on the older side of the typical age range for BOC. The site and the clinical presentation of pushing teeth apart are consistent with BOC; the delayed recurrence is also consistent with BOC.
The histology showed epithelium that is of variable thickness with two epithelial spherules, making it difficult to definitively exclude BOC as part of the final diagnosis. The histology is therefore focally suggestive of BOC.
Sorry, you are incorrect!
A well-demarcated radiolucent lesion between teeth involving the full-length of the roots should also include OKC on the DDX list. The site in the anterior jaw is less consistent with this condition, since OKCs are more common in the posterior mandible and ramus area, and only occur in the anterior jaws in about 7% of cases. Because OKCs occur in a wide age range, the older age of the patient in this case is not unusual. The recurrence after 22 years is also consistent with the behavior of this cyst since OKCs have a tendency for late recurrence; this reviewer has seen an OKC recur as late as after 26 years. The mild expansion and pushing of teeth apart is unusual with smaller OKCs, and the lesion in this case would be considered small if it were an OKC. However, large OKCs can push teeth apart and cause expansion. The histology in this case is not consistent with OKC.
Sorry, you are incorrect!
The site anterior to the mandibular first molar, the radiographic changes, and the mild pushing of teeth apart are all consistent with the clinical and radiographic occurrence of CGCG. The patient’s gender and age, however, are not consistent with CGCG. About 60% of CGCG cases occur in patients under 30 years of age, with a predilection for occurrence in females. The histology of this case is not consistent with CGCG.
Congratulations, you are correct!
Although all of the clinical findings in this case are not consistent with unicystic ameloblastoma, the histology is, and so is the radiographic finding of a well-defined unilocular radiolucency between teeth. The patient’s age, the site, and the recurrence after 22 years are all not consistent with UA. The age of this patient is above the age range of typical occurrence; UAs located
between teeth constitute less than 10% of all cases; and the anterior mandible is a very rare site for UA. Unicystic ameloblastomas radiographically unilocular and are associated with the crown of an impacted third molar in the mandible in 90% of cases. The other 10% are unilocular radiolucencies usually associated with teeth, including between teeth as is the case in this patient. The age of UA patients is much younger than this patient now or in 1996. The typical age range is 10-20 years. UAs can loosen, displace and resorb adjacent teeth. Curettage is the treatment of choice for UA, especially the luminal histologic subtype, which has an approximately 7% recurrence rate. It is highly unusual for UA to recur after 22 years, but it did in this case.
The morphology of the associated cyst is suggestive of lateral periodontal/botryoid odontogenic cyst favoring BOC over lateral as described under the DDX of BOC.