All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Large unilocular radiolucency with scalloped border, anterior mandible
Contributed by: Dr. Philip Chen
Bellingham Oral & Maxillofacial Surgery-WA
Case Summary and Diagnostic Information

This is a 44-year-old Caucasian male who was referred by his general dentist due to the incidental finding of a large radiolucency discovered on a routine periapical (PA) dental radiograph.
This is a 44-year-old Caucasian male who was referred by his general dentist due to the incidental finding of a large radiolucency discovered on a routine periapical (PA) dental radiograph. The patient denied any symptoms from the lesion; therefore, the duration is unknown. The oral surgeon took a panoramic radiograph (Figure 1) which showed a large radiolucency with a scalloped border between teeth #s 20 to 24.
Figure 1 Panoramic radiograph taken at first clinical presentation demonstrating a unilocular radiolucency with scalloped border squeezing between teeth in the anterior mandible between teeth #s 22 and 24.
The patient’s past medical history is unremarkable, and he is otherwise healthy.
The patient was referred to oral surgeon Dr. Phillip Chen for evaluation of the radiolucency. A panoramic radiograph showed a much larger radiolucency than that initially shown on the PA. Clinical examination showed no measurable bony expansion and no pain. Upon palpation, there was no discomfort and no tooth mobility. The radiolucency was scalloped and unilocular between teeth #s 20 and 24 (Figure 1).
Under IV sedation, a buccal vestibular incision was made in area of teeth #s 22 and 23. When the mucoperiosteal flap was raised, the surgeon noticed perforation of the lesion through the buccal bony plate. After gaining access to the lesion, the entire cyst was removed and the bone curetted. The cyst appeared to be even larger than suggested on the panoramic radiograph. It was submitted for histologic evaluation.
The H & E stained sections revealed a large cystic structure lined by epithelium and supported by a fibrous connective tissue wall (Figures 2-4). The lining epithelium was of variable thickness and had gland-like spaces within the epithelium (Figures 2-4), scant mucous producing cells which were positive with Mucicarmine stain (Figure 5), and cuboidal epithelial cells with a hobnail appearance layering the very superficial layer of the lining epithelium and epithelial spheres.
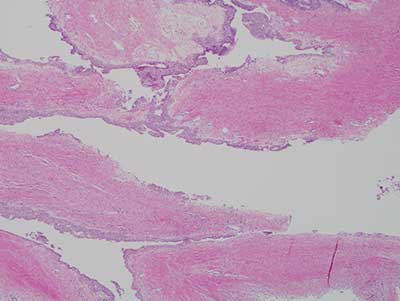
Figure 2 Low power (X40) histology shows H & E stained section shows a large and folded cystic structure with epithelium of variable thickness and prominent connective tissue wall.
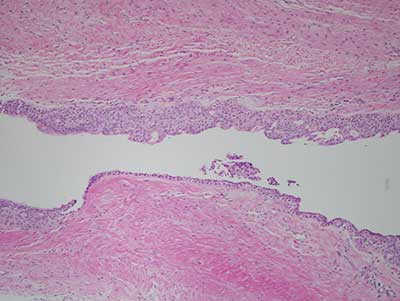
Figure 3 Higher power (X100) histology shows H & E stained section takes a closer look at the cystic structure with epithelium exhibiting micro-cystic spaces within the lining epithelium and cuboidal cell with hobnail appearance.
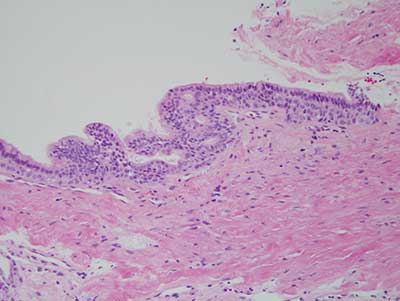
Figure 4 Higher power (X200) histology shows H & E stained section showing the lining epithelium with micro-cystic structures and hobnail cuboidal cell. The epithelium also showed focal proliferations forming epithelial spheres (not shown).
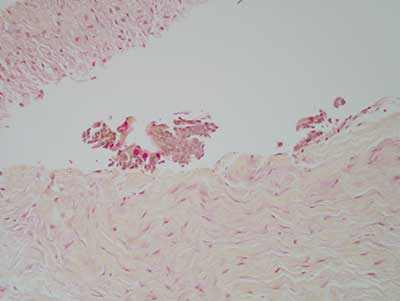
Figure 5 Higher power (X100) histology shows Mucicarmine stain, a special stain for mucous. This stain is positive for small clusters and isolated mucous producing cells within the lining epithelium.
After you have finished reviewing the available diagnostic information