Slowly Enlarging Lesion on the Right Lateral Tongue
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by Dr. Peter Van Der Ven
Oral & Maxillofacial Surgery, Lakewood, WA
Case Summary and Diagnostic Information

This is an 82-year old white male with a two-year history of a slowly enlarging lesion on the right lateral border of tongue.
Diagnostic Information Available
This is an 82-year old white male with a two-year history of a slowly enlarging lesion on the right lateral border of tongue. The lesion is well demarcated with rolled border. It is mostly pink and has a lobular/papillary appearance (Figure 1). There is a smooth white patch to its posterior. The lesion is described to be 1.3 x 1.8 cm in size and is “sore” but not painful. The patient’s past medical history is significant for cigarette smoking for approximately 30 years; however, the patient quit smoking 42 years ago.
Figure 1 This photograph represents the lesion at first clinical presentation. Note the circumscribed lesion on the right lateral border of tongue. The lesion has a rolled border and the center contains bluntly papillary pink soft tissue.
The patient’s past medical history is significant for cigarette smoking for approximately 30 years; however, the patient quit smoking 42 years ago.
The clinical examination revealed a well-demarcated pink and bluntly papillary lesion and rolled border present on the right lateral border of tongue (Figure 1). Distal or posterior to this lesion is a white patch that is smaller and is smooth surfaced. This lesion is 1.3 x 1.8 cm in size. It is not painful and has been present for two-years.
Figure 1 This photograph represents the lesion at first clinical presentation. Note the circumscribed lesion on the right lateral border of tongue. The lesion has a rolled border and the center contains bluntly papillary pink soft tissue.
Treatment
Two small punch biopsies were performed under local anesthesia (Figure 2).

Figure 2 This photograph represents the lesion stained with toluidine blue and punch biopsied at two separate poles (anterior and posterior).
Incisional Biopsy
Histologic examination reveals two hemisected pieces of soft tissue composed of surface epithelium exhibiting high-grade atypia and invading the underlying fibrous connective tissue and focally invading the underlying skeletal muscle bundles (Figures 3-5). The surface epithelium shows evidence of high-grade atypia manifested in loss of maturation, nuclear crowding, hyperchromatism and pleomorphism, readily identifiable mitotic figures and alteration in the nuclear/cytoplasmic ratio. Occasional atypical mitoses are also present. These changes are present within the surface epithelium in some areas and are invading the connective tissue in form of small nests and islands. The small nests have central keratin formation while the islands do not show obvious keratinization. The neoplastic islands are of variable shapes and sizes and invade the connective tissue and muscle (Figures 4-5).
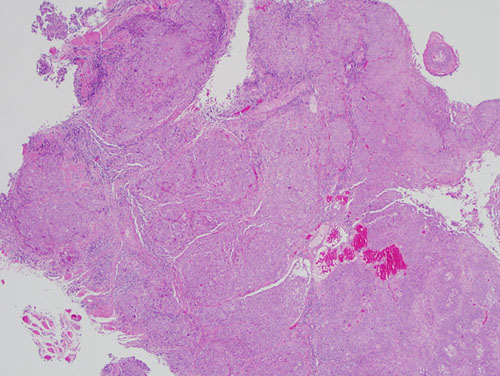
Figure 3 Low power (x100) H & E histology demonstrating neoplastic epithelial cells arranged in sheets and islands invading the connective tissue and the underlying skeletal muscle bundles.
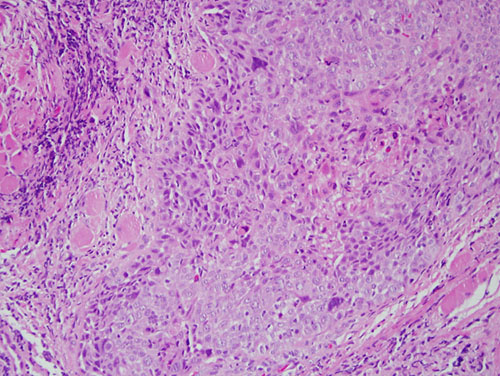
Figure 4 Higher power (x200) H & E histology demonstrating neoplastic epithelial cells arranged in sheets and within the connective tissue and invading the underlying skeletal muscle bundles.
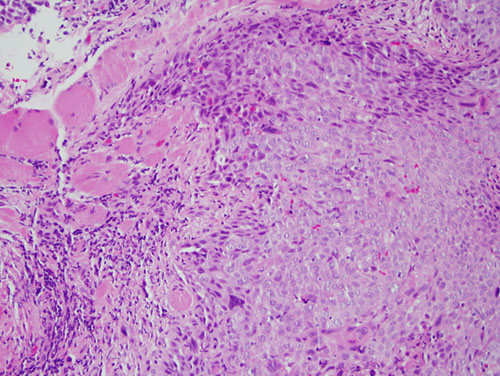
Figure 5 Higher power (x200) H & E histology at higher power.
After you have finished reviewing the available diagnostic information