Return to Case of the Month Archives
Diffuse, large swelling right palate
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. David Cotant
Oral & Maxillofacial Surgery, Lakewood, WA
Case Summary and Diagnostic Information

This is an 81-year-old white female whose chief complaint was that her partial denture was impinging on the right side of her palate, where a large swelling was identified. The palatal swelling was of one month’s duration. The partial denture pushed into the swelling, causing some tenderness in the area. The swelling was diffuse, soft and deep with red overlying mucosa and a groove (Figure 1). It was described to be 2.0 x 1.0 x 0.75 cm in size.
Diagnostic Information Available
This is an 81-year-old white female whose chief complaint was that her partial denture was impinging on the right side of her palate, where a large swelling was identified. The palatal swelling was of one month’s duration. The partial denture pushed into the swelling, causing some tenderness in the area. The swelling was diffuse, soft and deep with red overlying mucosa and a groove (Figure 1). It was described to be 2.0 x 1.0 x 0.75 cm in size.
Figure 1 This is a clinical photograph taken at the first clinical presentation; note the swelling at the right side of the hard palate with central groove.
Her PMH is significant for diabetes and follicular cell lymphoma.
At presentation, the patient was wearing a maxillary partial denture. The left posterior region was normal while the right posterior was swollen, mostly on the palatal side. The partial denture was pushing into this swelling creating a groove (Figure 1) which was a source of discomfort to the patient. The swelling was described to be 2 x 1 x 0.75 cm in size and was diffuse and soft and had no bony involvement as depicted by the panoramic radiograph of fully intact alveolar/palatal bone of the right palate (Figure 2)
Figure 1 This is a clinical photograph taken at the first clinical presentation; note the swelling at the right side of the hard palate with central groove.

Figure 2 This is a panoramic radiograph taken at the first clinical presentation. The radiograph demonstrates an intact alveolar and palatal bone with no evidence of bony invasion
Treatment
Under local anesthesia, an incisional biopsy was performed and the tissue submitted for histologic evaluation.
Incisional and excisional biopsy
Histologic examination of the H & E sections showed sheets of monotonous, nodular, atypical lymphoid infiltrate. The atypical cells were predominantly small, with round to irregular nuclear contours, clumped chromatin and inconspicuous nucleoli. Scattered large cells with vesicular chromatin and one or more nucleoli morphologically consistent with centroblasts were identified. Using the Mann-Berard criteria counting 15 fields yielded an average of 7 centroblasts per field.
The immunohistochemical stains were positive for CD10, CD20 and BCL-2.
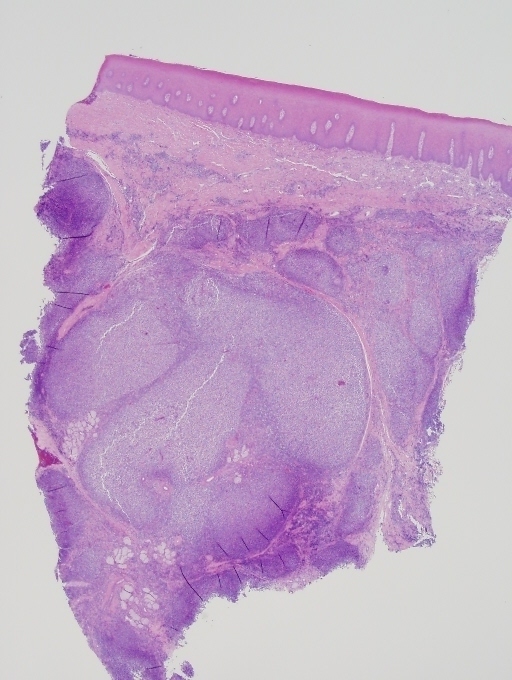
Figure 3 Low power (x40) H & E histology demonstrates a piece of mucosa infiltrated by sheets of monotonous, nodular, atypical lymphoid cells. They were predominantly small, with round to irregular nuclear contours, clumped chromatin and inconspicuous nucleoli. Scattered large cells consistent with centroblasts were also identified.
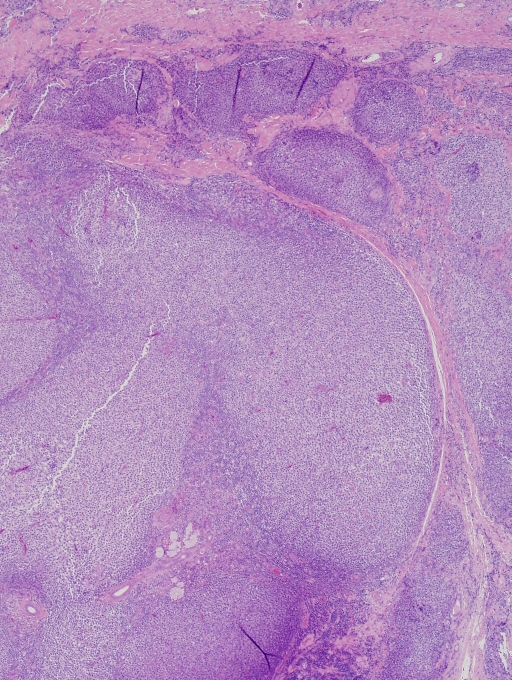
Figure 4 Higher power (x100) H & E histology demonstrates closer look at the atypical lymphoid cells arranged in lobules of predominantly small cells with round to irregular nuclear contours, clumped chromatin and inconspicuous nucleoli. Scattered large cells consistent with centroblasts were identified.
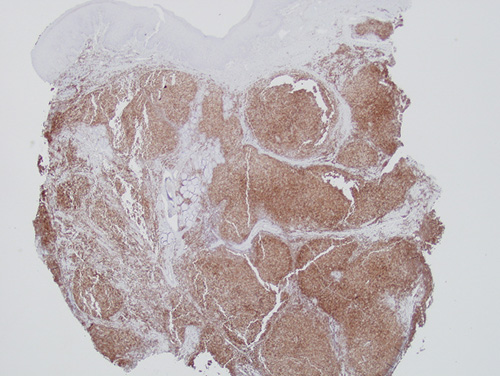
Figure 5 Low power (x40) Immunohistochemistry stain demonstrate that the atypical lymphoid cells are uniformly positive with BCL-2.
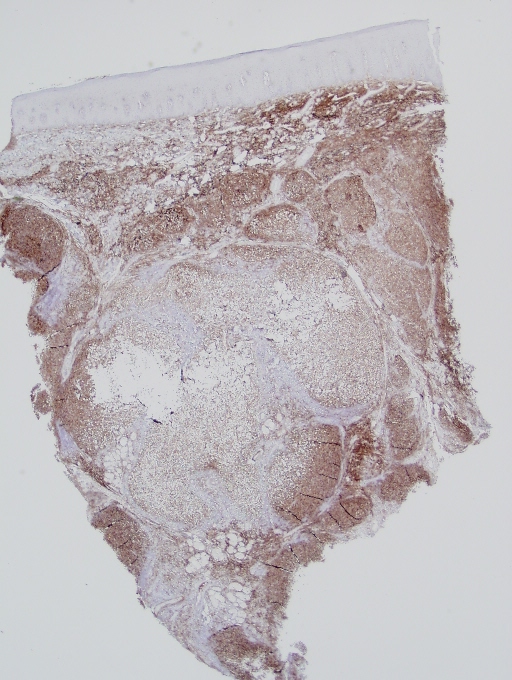
Figure 6 Low power (x40) Immunohistochemistry stain demonstrate that the atypical lymphoid cells are uniformly positive with CD-10. The CD10 positive B cells are noted not only within neoplastic follicles but are also increased within the interfollicular areas
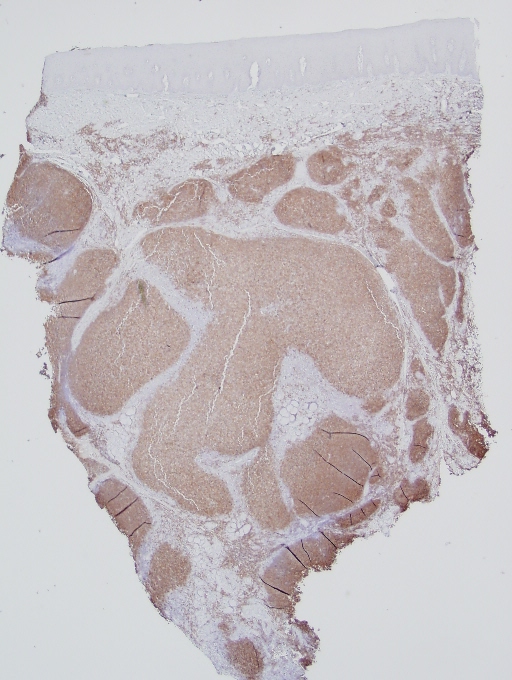
Figure 7 Low power (x40) Immunohistochemistry stain demonstrate that the atypical lymphoid cells are uniformly positive with CD-20.
After you have finished reviewing the available diagnostic information