All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Unilocular radiolucency with flecks of radiopacity between teeth #s 6 & 7
Contributed by: Dr. Jeremiah Johnson
Wenatchee Oral & Maxillofacial Surgery, WA
Case Summary and Diagnostic Information

This is a 14-year-old female who was referred by Dr. Johnson for the evaluation of a lesion in the right maxilla noted on a periapical radiograph after her general dentist noted loss of keratinized tissue with gingival erythema around tooth #7.
This is a 14-year-old female who was referred by Dr. Johnson for the evaluation of a lesion in the right maxilla noted on a periapical radiograph (Figure 1) after her general dentist noted loss of keratinized tissue with gingival erythema around tooth #7. Clinical examination at that time revealed a non-tender swelling in the right maxillary alveolus.
Figure 1 This is a periapical radiograph taken at the patient’s first presentation demonstrating a well-demarcated, unilocular radiolucency between teeth #s 6 & 7 with flecks of radiopacity.
The past medical history is unremarkable.
The clinical examination revealed mild buccal swelling in the right maxilla between teeth #s 6 and 7 (Figure 1). The radiograph demonstrates a well-defined unilocular radiolucency with flecks of radiopacity. The teeth are mildly displaced and are vital.
The procedure was performed under IV sedation. A subperiosteal flap was raised in the right maxilla (Figure 2) to expose the labial alveolar bone. The bone was partially removed enough to expose the lesion. The tumor was solid and well-circumscribed (Figure 3) and was enucleated with peripheral ostectomy. The residual alveolar defect was irrigated and grafted with bone allograft and covered with a collagen membrane. The surgical site was closed with 4-0 polyglactin sutures. At the two week post-operative visit the patient demonstrated normal healing.

Figure 2 This is an intra-oral photograph demonstrating a full-flap surgical procedure exposing the lesion buccally as the neoplasm is curetted out of the cavity.

Figure 3 This is the gross appearance of the enucleated lesion. It is round and encapsulated.
The biopsy revealed an encapsulated neoplasm of odontogenic epithelial origin. It is surrounded by dense fibrous connective tissue wall. The neoplasm is made up of epithelial cells arranged in strands, whorls (epithelial spheres) and duct-like structures (Figures 4-6). Small clusters of calcified material are also present (Figure 6) which explains the radiographic changes of flecks of calcification present within the radiolucent lesion.
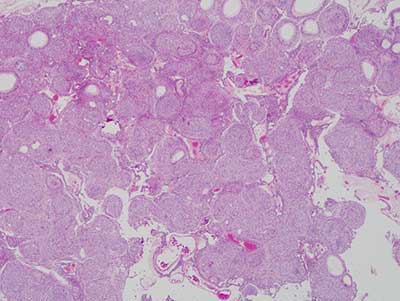
Figure 4 This is an H & E stained section at x 40 magnification demonstrating sheets of epithelial cells some are spindle-shaped, others are arranged in spherules and others are arranged in duct-like structures lined by cuboidal epithelial cells.

Figure 5 This is an H & E stained section at x 100 magnification demonstrating closer look at the duct-like structures and the epithelial spherules suspended on delicate collagen fibers.
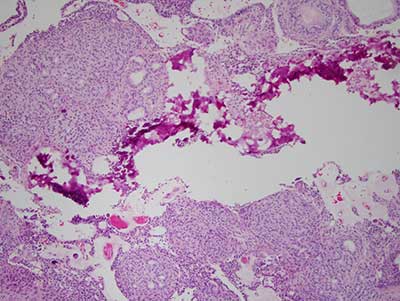
Figure 6 This is an H & E stained section at x 100 magnification demonstrating clusters of calcified material corresponding to the radiographic findings of flecks of radiopacity.
After you have finished reviewing the available diagnostic information