Large & Ulcerated Swelling on the Posterior/Lateral Palate
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by Drs. Jessica Lee & Namou Kim
Oral & Maxillofacial Surgery, Burien, & Swedish Medical Center, WA
Case Summary and Diagnostic Information

This is a 52-year-old male who presented with a swelling “lump” on the posterior/lateral junction of hard and soft palate, present for many years.
Diagnostic Information Available
This is a 52-year-old male who presented with a swelling “lump” on the posterior/lateral junction of hard and soft palate, present for many years (he doesn’t remember for how long, but he speculates at least 20 years). The swelling did not bother him until a few months ago when it suddenly started to grow and cause some discomfort and speech impairment. He also noticed that the swelling developed an area of surface ulceration (Figure 1). The surface ulceration and discomfort prompted him to seek care. The MRI (with contrast) image shows a well-demarcated solid soft tissue lesion that is mildly eroding the palatal bone (Figure 2).
Figure 1 This is a clinical photograph taken at the first clinical presentation; note the large exophytic and smooth-surfaced nodule in the right posterior junction of hard and soft palate. Also, note the ulceration close to the midline palate.
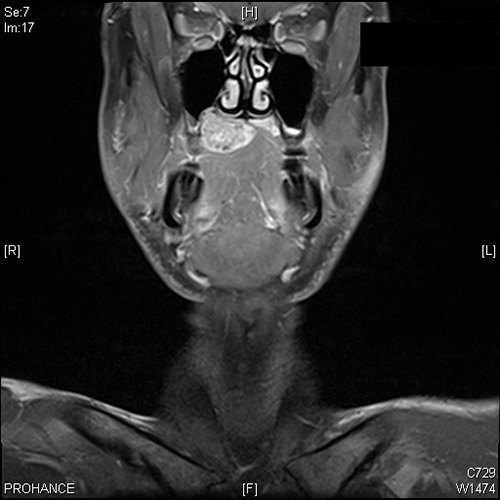
Figure 2 This is an MRI with contrast image taken at the first clinical presentation; note the large and well-demarcated soft tissue lesion mildly eroding the palatal bone.
The patient’s past medical history is unremarkable and the patient is otherwise healthy. The past medical history is negative for tobacco or alcohol use.
The patient reported a slowly enlarging lesion over a long period of time, estimated at 20-year period with recent discomfort and focal surface ulceration. The swelling is firm and well-demarcated both clinically and by MRI imaging.
Treatment
Under local anesthesia, an incisional biopsy was performed and based on the biopsy results, the lesion was completely excised.
Excisional Biopsy
Histologic examination reveals a large and multisected piece of soft tissue composed of ulcerated surface epithelium with underlying fibrous connective tissue almost all occupied by a neoplasm of salivary gland origin (Figures 3-5). The neoplasm is infiltrative (Figure 4) and is made up of two cell populations (Figure 3-5). The neoplasm is multinodular and is partially encapsulated. The neoplasm is made up of duct-like structure lined by two cell populations; the inner layer is made up of cuboidal cells with abundant cytoplasm and the outer layers are made up of cuboidal cells with clear cytoplasm (Figure 5). The latter cell population predominates. The neoplasm invades the surrounding connective tissue in multiple areas, some extending into the ulcerated surface epithelium.
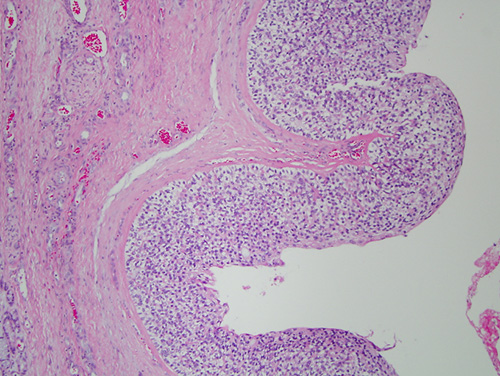
Figure 3 Low power (x40) H & E histology demonstrates a well-demarcated to partially encapsulated neoplasm of salivary gland origin. It is large and multinodular. It is biphasic in morphology but the clear cells predominate. It is infiltrative in multiple areas.
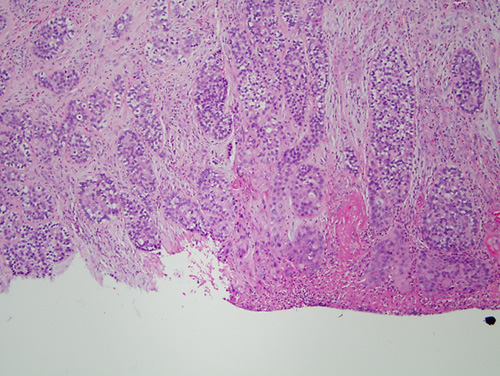
Figure 4 Higher power (x100) H & E histology demonstrates a closer look at the infiltrative neoplastic cells forming ducts with biphasic cellular morphology.
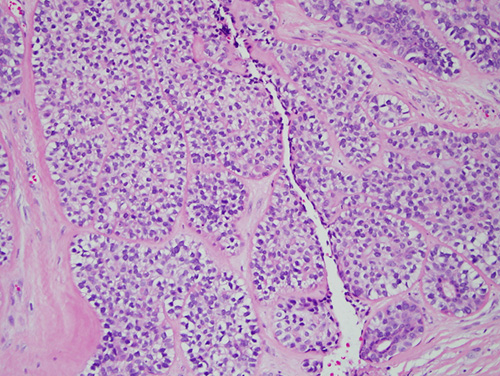
Figure 5 Higher power (x200) H & E histology demonstrates a higher magnification of the neoplastic cells with biphasic cell morphology.
After you have finished reviewing the available diagnostic information