Single swelling hard palate, right side
Can you make the correct diagnosis?

This is a healthy 15-year-old Caucasian girl who first presented to the University of Washington Pediatric clinic with slight mucosal thickening and swelling in the right hard palate below teeth #s 4 & 5.
Sorry! you are incorrect
The epithelial thickening description may suggest focal epithelial dysplasia. However, neither the location nor the isolated mass-type presentation is supportive of focal epithelial hyperplasia. The histology was not supportive of this diagnosis.
Focal epithelial hyperplasia, also known as Heck’s disease, is common among Native Americans, predominantly within the South American population (1). It is rare in Caucasian and black populations. It is induced by human papilloma virus (HPV) types 13 and 32. It was first described by Archard et al in the Eskimo population of the Greenland area. It has a distinct presentation (1-3). Occurring in children living in poor conditions, it presents in multiple small (around 5mm or slightly larger) slightly elevated, smooth-surfaced and dome-shaped nodules, pink in color, similar to the surrounding mucosa (1, 2). These lesions can be isolated or coalesced, forming a more diffuse and ill-defined elevation of the mucosa. Lip and buccal mucosa are the most common locations, but they can also occur on the gingiva, palate and other areas (1-3). A similar lesion has been described in AIDS patients; some are also HPV 13 and 32 positive (1). Histologically, they present as blunt dome-shaped epithelial hyperplasia with mitosoids (the latter are not always present). Treatment includes observation, because these lesions can spontaneously regress. Others respond to laser treatment. Alternative forms of therapy include intralesional injections or topical chemotherapy (2). The lesions in AIDS patients can be resistant to treatment (1).
Congratulations! You are correct
Although the location is unusual for granular cell tumor; the histology was that of this condition. This is a benign neoplasm of nerve origin supported by Immunohistochemistry markers (4). The tongue is the most common site of occurrence of this tumor; almost a third of the cases occur in the tongue, more dorsal-lateral than ventral. Although skin is another common site, it can occur in a variety of sites and tends typically to be benign. A malignant form, though described, is rare.
In the mouth, the buccal mucosa is second to the tongue in site predilection (5-6). Hard and soft palate and the gingiva are rare locations for granular cell tumor, but they have been described (4-6). This lesion is more common in females than males (2:1 ratio). Although it typically occurs in adults over 30, it has also been described in children of an average age of 14.5 in a 3-19 range (5). In children it is 3:1 females and has a 50% occurrence in the tongue (6). It is usually asymptomatic and can be of a long-term duration, ranging from months to years. The dorsal-lateral tongue is a common location; in about 80% of cases it is superficial and submucosal. The color ranges from pink or white with a keratotic surface to yellow-orange. A newborn counterpart is described and is known as congenital epulis of the newborn; it is believed to be a separate entity with different cell origin.
Histologically, granular cell tumor is composed of strands and fascicles of large cells with distinct cell borders containing abundant granular cytoplasm (4-6). The nuclei are small and round to oval and are eccentrically located. These cells are at times intimately related to surrounding skeletal muscle fibers and at times to nerve. The lesion can be well demarcated and confined or infiltrative. The overlying epithelium can be normal in thickness or proliferative with pseudoepitheliomatous hyperplasia (PEH) (4-6). The latter, when extensive in rare cases, can be mistaken for well differentiated squamous cell carcinoma, especially if the biopsy is superficial.
The tumor cells are positive with S-100 protein and neuron specific enolase (NSE) indicating a neural crest origin. Treatment includes conservative surgical excision. Recurrence is extremely rare.
Treatment
Under general anesthesia, the lesion was completely excised down to the periosteum with clean margins leaving the bone intact (Fig 2). The tumor was removed intact as one specimen. The Bovie electrocautery was used in the surgical area to obtain hemostasis. The area was irrigated multiple times and packed with bacitracin ointment soaked iodoform gauze, which in turn was secured with a prefabricated dental splint fastened by wires. The area healed well within one week post surgery. The splint was removed and the area granulated well.
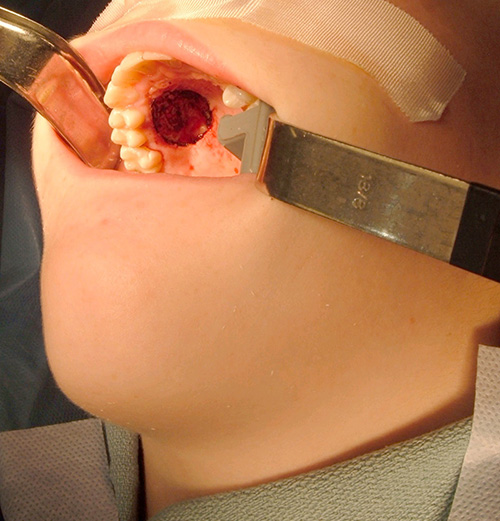
Figure 2. This is a clinical photograph of the surgical area after the lesion was completely excised in one piece.
References
- Garcia-Corona C, Vega-Memije E, Mosqueda-Taylor A, Yamamoto-Furusho JK, Rodriguez-Carreon AA, Ruiz-Morales JA, et al. Association of HLA-DR4 (DRB1*0404) with human papillomavirus infection in patients with focal epithelial hyperplasia. Arch Dermatol. 2004 Oct; 140(10):1227-31.
- Akyol A, Anadolu R, Anadolu Y, Ekmekci P, Gurgey E, Akay N. Multifocal papillomavirus epithelial hyperplasia: successful treatment with CO2 laser therapy combined with interferon alpha-2b. Int J Dermatol. 2003 Sep;42(9):733-5
- Jayasooriya PR, Abeyratne S, Ranasinghe AW, Tilakaratne WM. Focal epithelial hyperplasia (Heck’s disease): report of two cases with PCR detection of human papillomavirus DNA. Oral Dis. 2004 Jul;10(4):240-3
- Brannon RB,Anand PM. Oral granular cell tumors: an analysis of 10 new pediatric and adolescent cases and a review of the literature. J Clin Pediatr Dent. 2004; 29(1):69-74.
- Boulos R, Marsot-Dupuch K, De Saint-Maur P, Meyer B.Granular cell tumor of the palate: a case report. AJNR Am J Neuroradiol. 2002 May; 23(5):850-4.
- Bernat Gili A, Ayerbe TV, Baena AA, Rivares EJ. Abrikosoff’s tumor of the soft palate. A case report. An Otorrinolaringol Ibero Am. 1999;26(1):47-53
- Bentz BG, Hughes CA, Ludemann JP, Maddalozzo J. Masses of the salivary gland region in children. Arch Otolaryngol Head Neck Surg. 2000 Dec; 126(12):1435-9.
- Waldron CA. Mixed tumor (pleomorphic adenoma) and myoepithelioma. In Ellis GL, Auclair PL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: W.B. Saunders, 1991. p. 165-186.
- Hockstein NG, Samadi DS, Gendron K, Carpentieri D, Wetmore RF. Pediatric submandibular triangle masses: a fifteen-year experience. Head Neck. 2004 Aug; 26(8):675-80.
- da Cruz Perez DE, Pires FR, Alves FA, Almeida OP, Kowalski LP. Salivary gland tumors in children and adolescents: a clinicopathologic and immunohistochemical study of fifty-three cases. Int J Pediatr Otorhinolaryngol. 2004 Jul; 68(7):895-902.
- Shafer WG. Verruciform xanthoma. Oral Surg Oral Med Oral Pathol. 1971; 31:784-789.
- Philipsen HP, Reichart PA, Takata T, Ogawa I. Verruciform xanthoma–biological profile of 282 oral lesions based on a literature survey with nine new cases from Japan. Oral Oncol. 2003 Jun; 39(4):325-36.
Sorry! you are incorrect
The middle hard palate is an unlikely location for a salivary gland neoplasm. Usually, the salivary gland neoplasms occur in the lateral posterior hard palate and anterior lateral soft palate. The age of the patient is also unusual for MT. However, palatal swelling in children should always be taken seriously and salivary gland neoplasm should be ruled out through a biopsy. Mucoepidermoid carcinoma is the most common malignant salivary gland neoplasm in children. The color and the consistency of this swelling were not supportive of the clinical presentation of a mucoepidermoid carcinoma. The color and the firm consistency is more likely to be a mixed tumor. The histology was not supportive of a salivary gland neoplasm.
Pleomorphic adenoma is the most common benign salivary gland neoplasm of both the major and minor salivary glands. It originates from the myoepithelial and reserve cells of the intercalated ducts. It accounts for 80% of all benign salivary gland neoplasms. It occurs in both major and minor salivary glands and accounts for up to 77% of parotid, 68% of submandibular, and 43% of minor salivary gland tumors (50). Although most common in females 30-50 years of age, it is also described in children (7, 10). One study reports 1% of cases affecting children under 10 years of age and 5.9% between the ages of 10-20 (7). It presents as a small, painless, slowly enlarging nodule. If left untreated it can enlarge significantly, sometimes increasing by several pounds in weight (7-10). It occurs in the oral cavity, especially the palate and lips (7-10). The hard palate mixed tumor is fixed due to the bone-bound anatomy of the region. The tumor is otherwise movable. The behavior of the tumor in children is similar to that in adults (7). Histologically, the mixed tumor has a wide variety of cellular and pattern manifestations; the main cellular components are epithelial duct-like structures and mesenchymal-like tissue such as myxochondroid matrix. These lesions are generally encapsulated, ranging from predominantly myxoid (36%) to extremely cellular (12%) (8-9). Complete surgical removal with clean margins is the preferred treatment (7-10). Palatal lesions respond well to excision in one piece with the periosteum and overlying mucosa. Prognosis is good, but it has a tendency for recurrence (up to 44%) if not treated thoroughly. Risk of recurrence is less with minor salivary glands (up to 20%). The risk of malignant transformation is about 5% (7).
Sorry! you are incorrect
The palate and gingiva are common locations for verruciform xanthoma, and for that reason it would be a good condition to be included on the differential diagnosis. The color is not supportive, although at times VX can be pink in color. The histology was not supportive of this condition.
Verruciform xanthoma is a benign condition of unknown etiology and pathogenesis but is favored to be an inflammatory process rather than a neoplasm (11). Viral etiology has been suggested, especially in association with human papilloma virus (12). It has been described in connection with oral lichen planus, which is the case with this patient. It has also been described in association with recessive dystrophic epidermolysis bullosa, graft vs. host disease, congenital hemidysplasia with ichthyosiform erythroderma and limb defect (CHILD) syndrome, and epidermal nevus.
VX was first described in the oral cavity by Shafer et al in 1971 (11), and has since been reported in many other areas including the anogenital area and skin (11-12). VX usually presents as a solitary lesion but can also present in multiples. It ranges in diameter from a few millimeters to two centimeters (cm) with an average size of 1cm. However, larger VXs of several cms in size have been described. They can be flat or raised and warty and can be reddish-pink, yellow, orange, white or gray.
VX is most commonly described in patients in the fifth and sixth decade of life with a 2:1 predilection for occurrence in females (11-12). VX of the scrotal area is described mostly in older Japanese males with a wide age range. It is rare in children in general. It is usually asymptomatic and does not have a specific clinical presentation. However, when presenting as yellowish or orange-like in color, it can be clinically diagnostic. It can occur anywhere in the mouth, but the gingiva and the alveolar ridge constitute 50% of all cases, followed by the palate. The tongue is a rare location for VX (11-12).
The histology is characterized by papillary epithelium with evenly aligned rete pegs. The papillary projections are short, extending slightly above the surface. The projections have deep clefts filled with keratin. They are supported by connective tissue papillae, which are densely packed with large cells with foamy cytoplasm that are referred to as xanthoma cells. The latter are usually in the connective tissue papillae, but can extend into the surface epithelium and into the connective tissue below the superficial papillae. The xanthoma cells are believed to be of monocyte-macrophage lineage. Inflammatory cells and microabscesses can be present within the epithelium as well as the connective tissue.
Treatment consists of simple excision and recurrence is rare.