Return to Case of the Month Archives
December 2009: Large, unilocular and corticated radiolucency, left angle of mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. William C Colwell
Northgate Oral & Maxillofacial Surgery
Case Summary and Diagnostic Information
This is a 62-year-old male who presented complaining of “pain and swelling” in his left cheek. The patient was prescribed antibiotics for one week.
Diagnostic Information Available
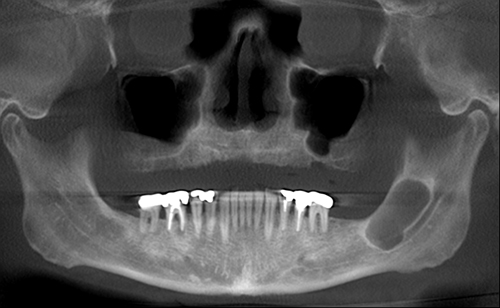
This is a 62-year-old male who presented complaining of “pain and swelling” in his left cheek. The patient was prescribed antibiotics for one week. Clinically, the swelling was not in the soft tissue but involved the angle of the mandible and part of the ramus. A panoramic radiograph revealed a large, corticated and unilocular radiolucency in the left mandibular angle and ramus (Figure 1). The radiolucency was surrounded by reactive bone formation. The patient’s past medical history is significant for one-pack-per-day cigarette smoking and Hepatitis C diagnosed nine years ago.
Figure 1 Panoramic view at first presentation demonstrating large unilocular radiolucency with corticated border involving angle of the mandible and part of the ramus.
The patient’s past medical history is significant for one-pack-per-day cigarette smoking. His PMH is also significant for Hepatitis C diagnosed nine years ago.
The panoramic radiograph demonstrates a well-defined and corticated unilocular radiolucent lesion occupying a significant portion of the left mandibular angle and extending superiorly into the ramus (Figure 1). Additional radiographic images show that this lesion is not significantly expansile but appears to be breaking through the lingual bone. The radiolucent lesion is surrounded by reactive bone formation manifested in more sclerotic and radiopaque bone.
Figure 1 Panoramic view at first presentation demonstrating large unilocular radiolucency with corticated border involving angle of the mandible and part of the ramus.
Treatment
Under IV sedation, the area was dissected and cortical bone removed to reveal a large cystic cavity partially filled with white cheesy material. The cavity was thoroughly curetted and the specimen submitted for histological evaluation. The surgical area was thoroughly irrigated and the soft sutured. The patient was placed on Percocet. The patient healed with no complications.
Incisional Biopsy
The excisional biopsy demonstrated multiple fragments of soft tissue made up of a cystic cavity lined by keratinized epithelium and surrounding by fibrous connective tissue wall (Figure 2). The lining epithelium is uniformly thin and corrugated and covered by parakeratin and orthokeratin. The basal cell layer shows evidence of focal palisading and reverse polarization (Figures 3 & 4). The lumen is focally filled with keratin (Figure 5).
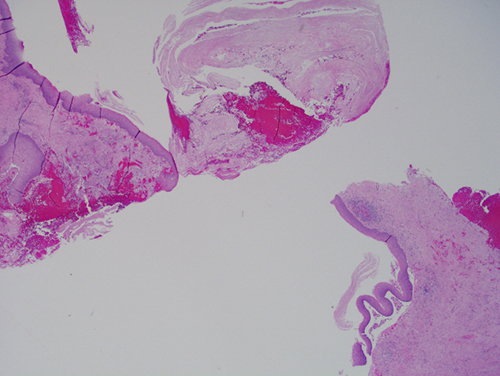
Figure 2 Low power (x40) histology shows a fragmented cystic structure with keratinized lining epithelium and connective tissue wall and keratin in the lumen.
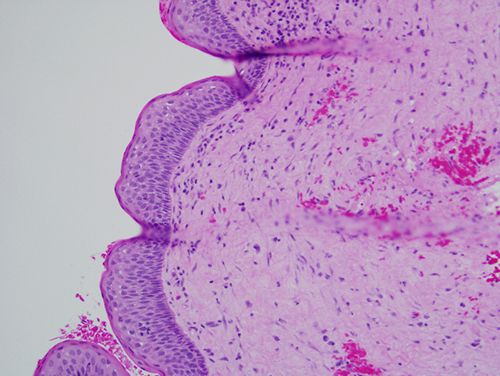
Figure 3 Higher power (x100) histology shows a uniformly thin, corrugated and keratinized lining epithelium with palisaded basal cell layer.
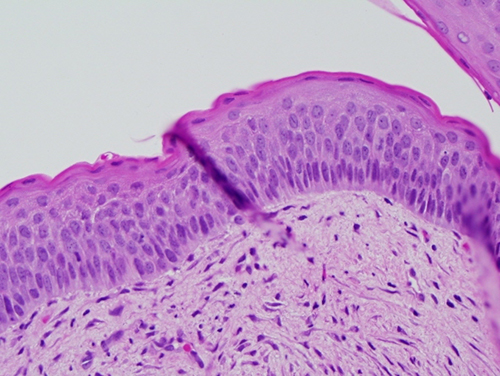
Figure 4 Higher power (x200) histology shows closer magnification of the palisaded basal cell layer with focal reversed polarization.
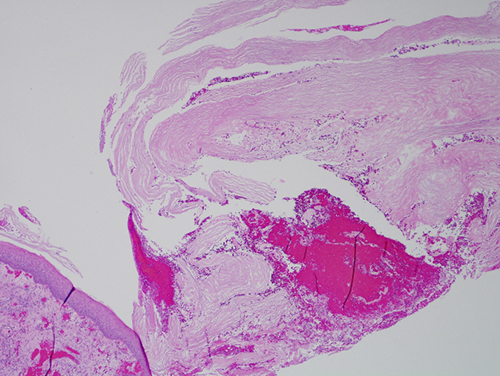
Figure 5 Low power (x100) histology shows a fragmented cystic structure with keratinized lining epithelium and keratin in the lumen.
After you have finished reviewing the available diagnostic information