All cases are discussed by: Dr. Dolphine Oda, UW-Oral Pathology Biopsy Service
Bilateral mandibular multilocular radiolucencies
Contributed by:
Dr. John Tidwell
Ballard Oral & Maxillofacial Surgery, Seattle WA
Case Summary and Diagnostic Information
This is an 11-year-old male who was referred to an oral surgeon by his pediatric dentist for evaluation of delayed eruption of teeth #s 18 and 31 and evaluation of bilateral, multilocular radiolucent lesions in the posterior mandible.

This is an 11-year-old male who was referred to an oral surgeon by his pediatric dentist for evaluation of delayed eruption of teeth #s 18 and 31 and evaluation of bilateral, multilocular radiolucent lesions in the posterior mandible (Figure 1). The patient reported no symptoms from the areas involved.
Figure 1 Panoramic view at presentation in October 2019 demonstrating symmetrical and bilateral multilocular radiolucency involving the first and second mandibular molars and extending posteriorly into the ramus.
The past medical history is unremarkable and there is no family history of related disease.
On clinical examination there was no obvious facial asymmetry and no paresthesia of the inferior alveolar or mental nerve distribution bilaterally. A panoramic radiograph showed delayed eruption of teeth #s 18 and 31 and adjacent impacted teeth #s 17 and 32. The radiograph also showed bilateral mandibular multilocular radiolucent lesions involving the posterior mandible and ramus. The lesions were more pronounced on the right side.
With IV anesthesia, a disto-buccal incision was made at 45 degrees toward the cheek from the middle of the mandibular second molars with full thickness mucoperiosteal flaps. The teeth were visualized, bone removed, and teeth sectioned to allow delivery of teeth. Curettage was performed and follicular tissue removed with care to avoid lingual and inferior alveolar nerves. Copious irrigation was followed by inspection of sockets. Gelfoam with doxycycline was placed in the lower sockets. Small fragments of tissue from the area of tooth #32 were submitted for microscopic examination.
Histologic specimens showed multiple small pieces of loose and cellular granulation tissue with clusters of multinucleated giant cells (Figures 2-3). Figure 4 shows multiple small blood vessels with a ring of hyalinized material frequently described in this condition.
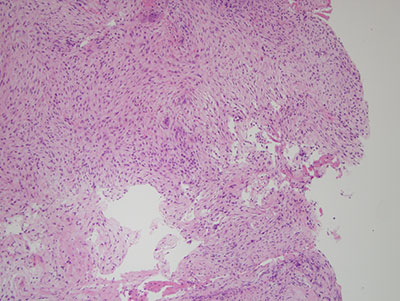
Figure 2 Low power (x100) histology shows cellular and myxoid granulation tissue background with many multinucleated giant cells and clusters of extravasated erythrocytes.
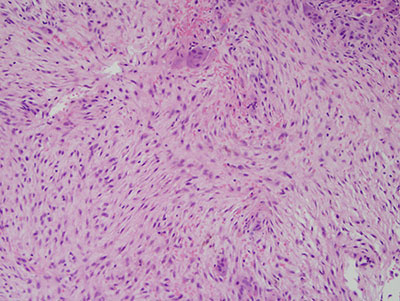
Figure 3 Higher power (x200) histology shows cellular granulation tissue with small clusters of multinucleated giant cells.
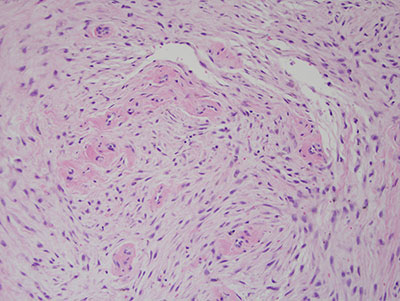
Figure 4 Higher power (x200) histology shows cellular granulation tissue with small blood vessels surrounded by a ring of hyalinized material.
After you have finished reviewing the available diagnostic information