Single Swelling on the Upper Lip
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by Dr. David Cotant
Oral & Maxillofacial Surgery, Lakewood, WA
Case Summary and Diagnostic Information

This is a 70-year-old male who presented with a smooth-surfaced, pink, firm nodule on the left side of the upper lip.
Diagnostic Information Available
This is a 70-year-old male who presented with a smooth-surfaced, pink, firm nodule on the left side of the upper lip (Figures 1& 2). The patient stated that it had been present for almost 20 years and had grown larger over the last few months. It is around 1.3 cm in diameter at its greatest dimension and is otherwise asymptomatic with an intact mucosa.
Figure 1. This photograph was taken at first clinical presentation and demonstrates a mild and localized swelling on the left side of the upper lip.

Figure 2. This photograph was taken at first clinical presentation with the clinician’s finger below the nodule on the left side of the upper lip.
The patient’s past medical history is significant for renal cell carcinoma treated five years ago. The patient is currently in remission.
The patient reported a nodule on his upper lip that was present for almost twenty years but started growing larger in the last a few months. The swelling was not painful and the overlying mucosa was intact.
Treatment
Under local anesthesia, an incision through the mucosa was performed where an encapsulated brown to purple nodule was released (Figure 3).

Figure 3. This photograph is of the gross specimen that shelled out easily. It is encapsulated, smooth-surfaced, brown to purple in color, and measures 1.3 x 1.3 x 1.0 cm at its greatest dimensions.
Excisional Biopsy
Histologic examination reveals a trisected piece of soft tissue composed of an encapsulated neoplasm of clear cell origin (Figures 4-6). The neoplastic cells are arranged in alveolar clusters surrounded by a prominent vascular component. The cells have clear cytoplasm and oval to round nuclei. They are well differentiated and show no evidence of atypia. The immunohistochemistry stain is positive with antibody to Pax8 (Figure 8) and pancytokeratin (Figure 7) and is negative with antibody to S-100, 1A4 (smooth muscle actin) and HMB 45/50.
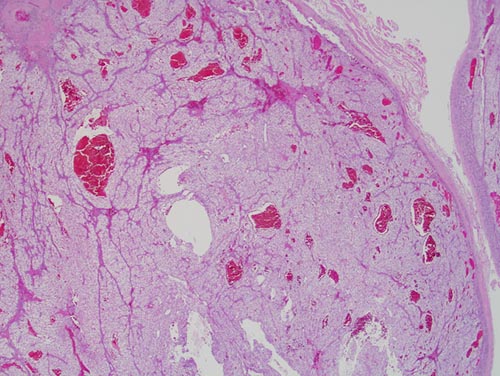
Figure 4. Low power (x40): the H & E histology reveals an encapsulated neoplasm of clear cell origin. The neoplastic cells are arranged in alveolar clusters surrounded by a prominent vascular component. The cells have clear cytoplasm and oval to round nuclei. They are well differentiated and show no evidence of atypia.
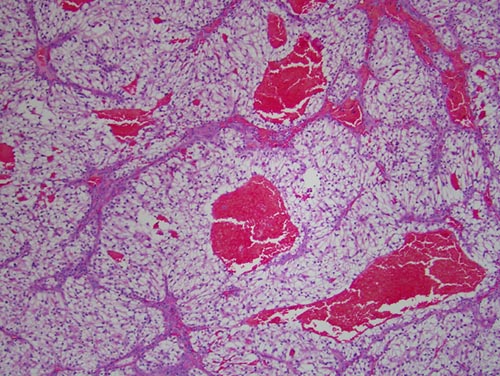
Figure 5. Low power (x100): the H & E histology reveals a neoplasm of clear cell origin. The neoplastic cells are arranged in alveolar clusters surrounded by a prominent vascular component. The cells have clear cytoplasm and oval to round nuclei. They are well differentiated and show no evidence of atypia.
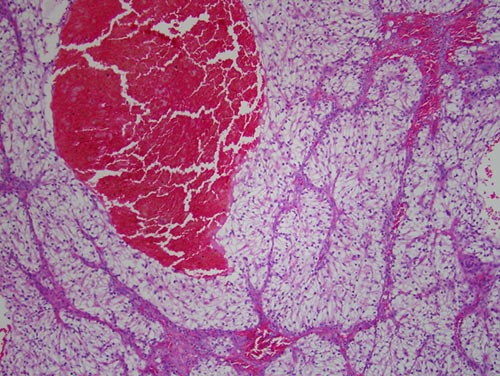
Figure 6. High power (x200): the H & E histology reveals a neoplasm of clear cell origin. The neoplastic cells are arranged in alveolar clusters surrounded by a prominent vascular component. The cells have clear cytoplasm and oval to round nuclei. They are well differentiated and show no evidence of atypia.
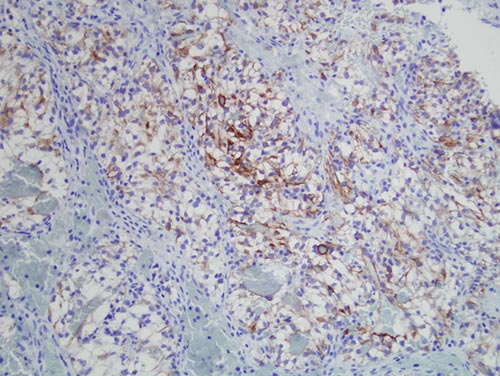
Figure 7. Low power (x100): the immunohistochemistry stain reveals the cytoplasm of the clear neoplastic cells to be positive with antibody to pancytokeratin (AE1/AE3).
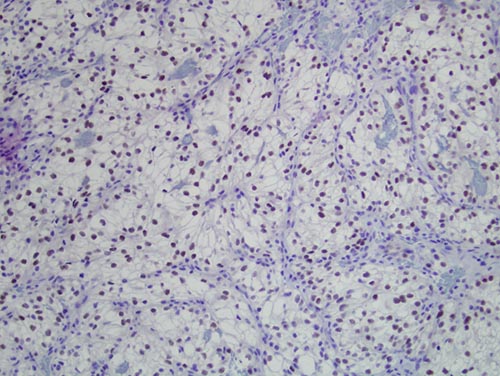
Figure 8. Low power (x100): the immunohistochemistry stain reveals the nuclei of the clear neoplastic cells to be positive with antibody to Pax8.
After you have finished reviewing the available diagnostic information