Generalized Ulcerative Palate and Maxillary and Mandibular Gingiva
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Earl Sommers
Department of Oral Medicine, University of Washington, Seattle, WA
Case Summary and Diagnostic Information

This is an 82-year-old white male who first presented to the UW otolaryngology clinic for ear pain, drainage and hearing loss.
Diagnostic Information Available
This is an 82-year-old white male who first presented to the UW otolaryngology clinic for ear pain, drainage and hearing loss. He was also complaining about generalized oral ulcers. He was referred to the oral medicine clinic at the UW School of Dentistry to evaluate generalized palatal and gingival painful ulcers (Figures 1-3) of at least six months duration. The ulcerated areas include the hard palate (Figure 1) and the maxillary (Figure 2) and mandibular (Figure 3) gingiva, both buccal/facial and lingual/palatal. The ulcers were mostly superficial and flat; however, in focal areas, especially on the palate, they were associated with swelling and had rolled borders. The ulcers are described as painful and persistent. The patient also complained of episodes of epistaxis and painful ears with drainage and hearing loss. The patient’s first oral biopsy showed lichenoid mucositis with tissue eosinophilia but the patient did not respond to the conventional treatment for lichen planus or lichenoid drug reaction. The lesions got progressively worse.
Figure 1. This photograph was taken at first presentation where diffuse superficial to focally rolled bordered ulcers are noted involving the hard palate and palatal gingiva.

Figure 2. This photograph was taken at first presentation where diffuse superficial ulcers are noted to involve the maxillary buccal gingiva.

Figure 3. This photograph was taken at first presentation where diffuse superficial ulcers are noted to involve the mandibular buccal gingiva.
The patient’s past medical history is significant for hypertension and stroke. The patient is on ACE inhibitors and antibiotics.
The generalized oral ulcers were progressive and painful. Though mostly superficial, they were preventing the patient from eating and from optimum oral hygiene care. As a result of the ulcers, he lost weight. The ulcerative lesions included those on the hard plate (Figure 1), the maxillary labial/buccal gingiva (Figures 2), and the mandibular labial/buccal and lingual gingiva (Figure 3). There was no evidence of vesicles, bullae, or of Nikolsky’s sign.
Figure 1. This photograph was taken at first presentation where diffuse superficial to focally rolled bordered ulcers are noted involving the hard palate and palatal gingiva.
Figure 2. This photograph was taken at first presentation where diffuse superficial ulcers are noted to involve the maxillary buccal gingiva.
Figure 3. This photograph was taken at first presentation where diffuse superficial ulcers are noted to involve the mandibular buccal gingiva.
Treatment
The patient was referred to an oncologist for treatment.
Excisional Biopsy
Histologic examination reveals two pieces of soft tissue composed of surface epithelium with underlying fibrous connective tissue intensely infiltrated by numerous eosinophils intermixed with sheets of histiocytes. Some have grooved nuclei consistent with Langerhans cell morphology (Figure 4), while some have large nuclei, prominent nucleoli, and readily identifiable mitotic activity not typical of Langerhans cell morphology or behavior. The Immunohistochemistry stain with Cd1a (Figure 5) and S-100 (Figure 6) antibodies were uniformly positive.
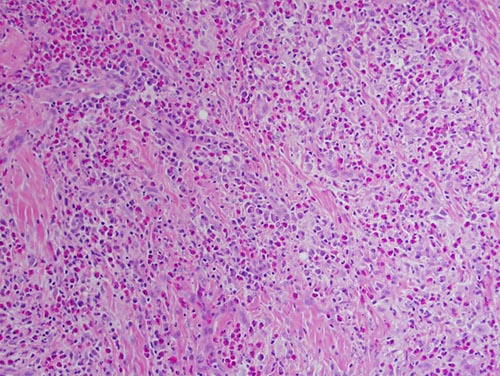
Figure 4. High power (x200) H & E stained histology shows a mass of vascular granulation tissue containing sheets of large “histiocytes” and large aggregates of eosinophils.
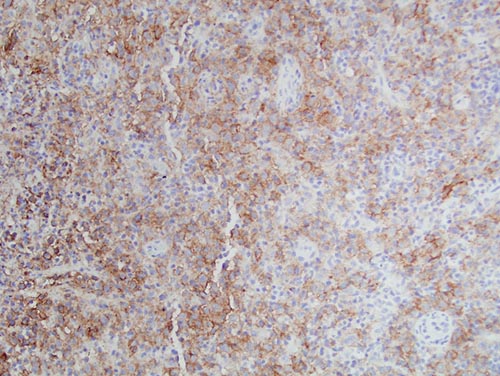
Figure 5. High power (x200) Immunohistochemistry stain with antibody to CD1a, the “histiocytes” were uniformly positive with this antibody.
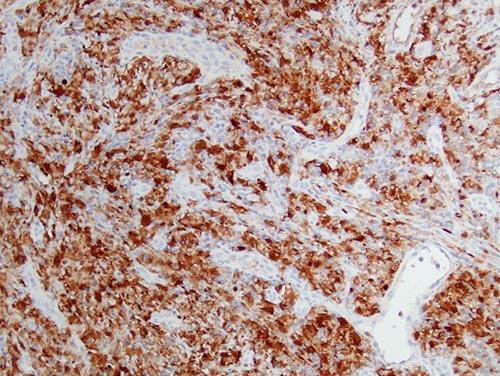
Figure 6. High power (x200) Immunohistochemistry stain with antibody to S-100, the “histiocytes” were uniformly positive with this antibody.
After you have finished reviewing the available diagnostic information