Return to Case of the Month Archives
Radiolucency anterior maxilla associated with impacted tooth #8
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. David Cotant, Andrew Leavitt, Gladys Semakula
Lakewood, WA
Case Summary and Diagnostic Information

This is a 12-year old African American female who was referred by her general dentist for orthodontic evaluation and treatment because of failure of the deciduous incisors to exfoliate and tooth #8 to erupt.
Diagnostic Information Available
This is a 12-year old African American female who was referred by her general dentist for orthodontic evaluation and treatment because of failure of the deciduous incisors to exfoliate and tooth #8 to erupt. The panoramic radiograph showed a fully impacted tooth #8 (Figure 1). The CT scan shows the tooth to be fully horizontal in the palate with the facial surface along the floor of the nose. There is a radiolucent lesion filling the anterior alveolus in the #8 area above the roots of the primary incisors. Within the lucency is a small round opacity.
The patient’s past medical history is negative; she has no known allergies and is not on any medications.
The panoramic radiograph (Figure 1) and subsequently the CT scan showed a horizontally impacted tooth # 8 and intact deciduous incisor. As demonstrated in Figure 1, the panoramic radiograph was not fully diagnostic of the position of the incisor. The CT scan shows that the tooth is fully horizontal in the palate with the facial surface along the floor of the nose. There is a radiolucent lesion filling the anterior alveolus in the area of tooth # 8 above the roots of the primary incisors. Within the lucency is a small round opacity.
Figure 1. This a panoramic radiograph at first presentation. Note the impacted tooth #8 surrounded by irregular radiolucency containing small foci of radiopaque material.
Figure 2. Kaposi’s sarcomas involving the soft palate and anterior hard palate. Note the purplish-red color, both are exophytic and the soft palate lesion is obstructive to the oropharynx.
Histologic evaluation revealed multiple small and decalcified pieces of hard and soft tissue made up of a combined benign odontogenic tumor and a pigmented odontogenic cyst (Figure 3). The cystic portion of this lesion is made up of lining epithelium of odontogenic origin containing clusters of epithelial ghost cells, melanin pigment and calcified material (Figure 4). Most of the latter is calcified ghost cells. Iron stain is negative for hemosiderin. The tumor is of mixed origin made up of primitive connective tissue with epithelial islands and areas of hyalinized connective tissue and dysplastic dentin and cementum (Figure 5).
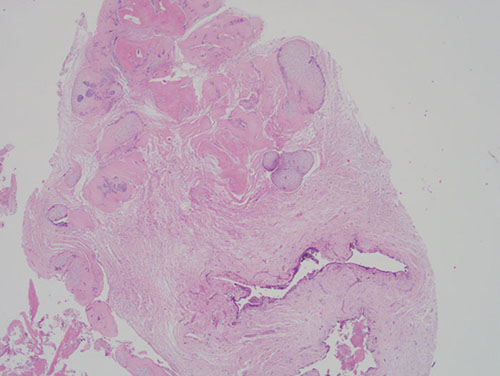
Figure 3. Low power (x100) histology shows a combined cyst and benign odontogenic tumor. The latter is of mixed epithelial and mesenchymal origin.
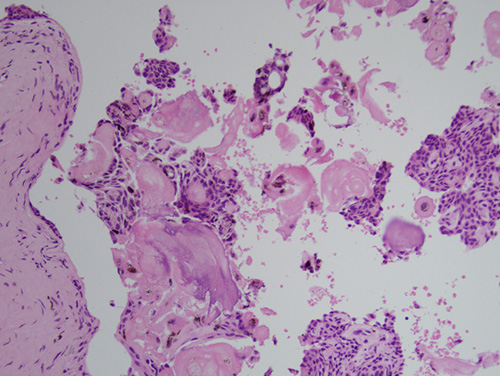
Figure 4. High power (x200) histology of the cystic structure shows odontogenic epithelial lining, ghost cells, connective tissue wall and melanin pigment.
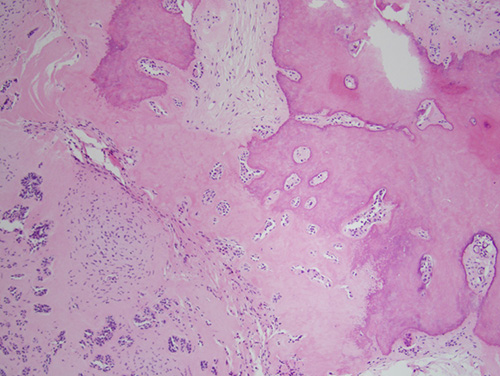
Figure 5. High power (x200) histology of the odontogenic tumor made up of primitive connective tissue stroma, epithelial islands and cords and dysplastic odontogenic hard tissue.
After you have finished reviewing the available diagnostic information