Large Swelling in the Left Floor of Mouth
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Dr. Brian Hart
Oral & Maxillofacial Surgery, Seattle, WA
Case Summary and Diagnostic Information

This is a 25-year-old male who presented with a mass of five years’ duration.
Diagnostic Information Available
This is a 25-year-old male who presented with a mass of five years’ duration. The mass was described to be slowly enlarging in size and was 1.5 x 1.5 x 1 cm at its greatest dimensions at the time of presentation. The mass was smooth-surfaced and pink to red in color with prominent surface vasculature (Figure 1). It was located below teeth #s 20-22. It was not painful and was firm on palpation.
Figure 1 This is a clinical photograph of the lesion at first presentation. It is present on the left side of the floor of mouth. Note the large, pink-reddish, smooth surfaced nodule with prominent surface vasculature.
This patient’s past medical history is not significant.
The patient presented with a five-year history of an enlarging mass in the left side of the floor of mouth. It was exophytic and smooth surfaced with prominent surface vasculature (Figure 1). On palpation, the nodule was firm. The color was pink to slightly red. There was no ulceration or purulent drainage. The swelling was about 1.5 cm in diameter.
Figure 1 This is a clinical photograph of the lesion at first presentation. It is present on the left side of the floor of mouth. Note the large, pink-reddish, smooth surfaced nodule with prominent surface vasculature.
Treatment
Under IV sedation, the lesion was completely excised. The lesion was firm to palpation. The surgical site was closed with Vicryl suture. The area healed with no complications.
Excisional Biopsy
Histologic examination reveals a multisected piece of soft tissue composed of a neoplasm of peripheral nerve origin. This neoplasm is encapsulated and is made up of two cell patterns (Figure 2). One of the patterns is composed of spindle-shaped cells arranged in bundles that are cross-sectioned, yielding Verocay bodies (Figure 3). The second cell population is also spindle-shaped but is not organized. It is haphazardly arranged. This neoplasm shows evidence of hyalinization, stromal hemorrhage yielding clusters of hemosiderin pigment, and cystic changes, all of which are consistent with degenerative changes that occur in chronic standing and traumatized lesions (Figure 4). It also contains dilated and congested small blood vessels. It is focally infiltrated by small clusters of lymphocytes.
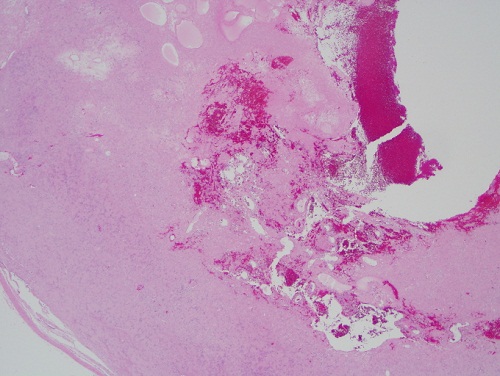
Figure 2 Screening power (x40) H & E stained section shows a large and encapsulated neoplasm demonstrating two patterns of histology (Antoni A & Antoni B) plus obvious cystic degeneration, hypocellularity and bleeding in the center of the neoplasm.
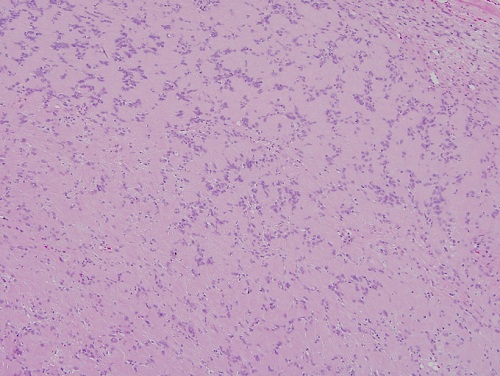
Figure 3 Low-power (x100) H & E stained section demonstrating bundles of spindle-shaped cells crisscrossing each other and forming Verocay bodies. Note at the upper right-hand corner the spindle-shaped cells are more haphazardly arranged.
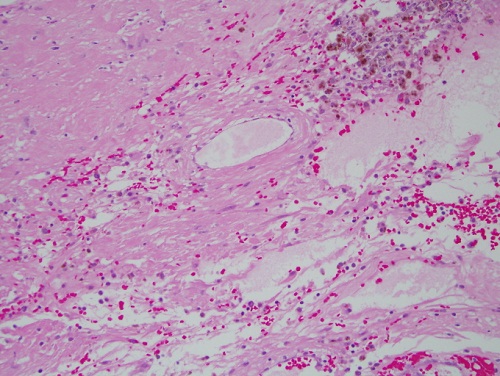
Figure 4 High-power (x200) H & E stained section shows a hypocellular area of the neoplasm. It also shows clusters of hemosiderin, degeneration and macrophages.
After you have finished reviewing the available diagnostic information