Large Ulcerated Swelling, Right Retromolar Pad & Tuberosity Area
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Craig Neal
Neal Oral & Maxillofacial Surgery, Seattle, WA
Case Summary and Diagnostic Information

This is a 15-year-old male who was referred for third molar removal to accommodate arch length deficiency.
Diagnostic Information Available
This is a 15-year-old male who was referred for third molar removal to accommodate arch length deficiency. All four third molars were extracted uneventfully. However, one week post-surgery, the patient presented with pain in the area of tooth #1. He was diagnosed with an infection and treated with antibiotics. The pain persisted, however. In the second week post-surgery, the patient presented with an ulcerated soft tissue swelling in the right retromolar pad region associated with trismus. The soft tissue swelling was surgically excised with a non-specific histology. It recurred after two more weeks, once again ulcerated and associated with trismus, and did not resolve. The second specimen was also excised and this time was noted to extend medially to the mandible.
Figure 1. Photograph is taken at second recurrence in October demonstrating a large, ulcerated and necrotic lesion in the right retromolar pad area and extending into the tuberosity area and anteriorly into the posterior buccal mucosa.
The patient’s past medical history is not significant.
The patient was referred for third molar removal. At presentation, he had class I occlusion, a lingual arch bar in place, and not all the third molars were visible. There was no swelling, no mass, and no trismus. The head and neck examination was otherwise normal. Things changed one week post-surgery as described in history of present illness.
Treatment
The earlier biopsies were performed under local anesthesia and the second biopsy was performed under general anesthesia. The patient was referred to Seattle Children’s Hospital for further evaluation and treatment.
Incisional Biopsy
The histological diagnosis was read by Dr. Thomas Morton, University of Washington, Oral Pathology Biopsy Service and Dr. Kathy Patterson, Seattle Children’s Hospital.
Histologic examination revealed ulcerated surface epithelium with underlying fibrous connective tissue infiltrated by small to medium blue cells with vesicular nuclei (Figure 2). The neoplastic cells are arranged in groups and strands separated by collagen fibers and small blood vessels (Figure 2). Mitotic figures and apoptotic cells are readily identifiable. The Immunohistochemistry staining shows diffusely positive nuclear MyoD staining (Figure 3) and positive staining with desmin (Figure 4).
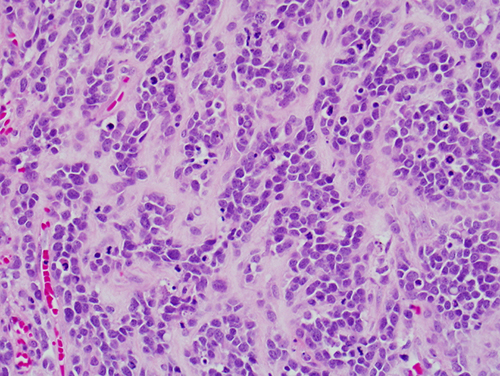
Figure 2. Low power (x400) the H & E histology reveals an infiltrative neoplasm made up of small to medium blue cells with vesicular nuclei arranged in groups and strands separated by collagen fibers. Mitotic figures and apoptotic cells are common.
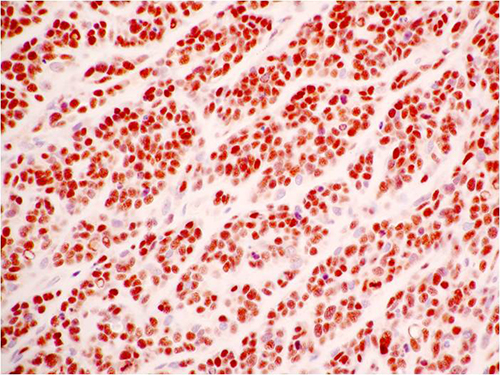
Figure 3. Higher power (x400) the Immunohistochemistry stain demonstrates small to medium sized neoplastic cells to be positive with antibodies to MyoD. The positive staining is nuclear.
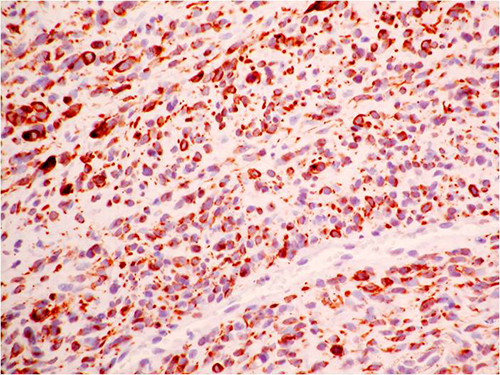
Figure 4. Low power (x400) the Immunohistochemistry stain demonstrated small to medium sized neoplastic cells to be positive with Desmin.
After you have finished reviewing the available diagnostic information