Return to Case of the Month Archives
Large Radiolucency, Right Posterior Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. John Evans
Department of Oral & Maxillofacial Surgery, UW, Seattle, WA
Case Summary and Diagnostic Information
This is a 54-year-old white male who was referred to the Department of Oral Surgery, UW SOD for a swelling in the right mandible involving teeth #s 29-32.
Diagnostic Information Available
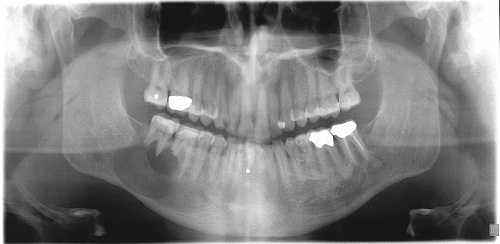
This is a 54-year-old white male who was referred to the Department of Oral Surgery, UW SOD for a swelling in the right mandible involving teeth #s 29-32. The panoramic radiograph demonstrates a large and well-defined unilocular radiolucency in the right posterior mandible of 1.5 to 2.0 cm in size (Figure 1). Distal to the large radiolucency and below the inferior alveolar canal is a much smaller round radiolucent lesion. The large lesion was buccally expansile and the lesion had perforated the buccal plate. There was little to no lingual plate in that area. Both teeth #s 30 & 31 showed evidence of resorption. The mesial root of tooth #31 was sharply resorbed.
Figure 1. Panoramic radiograph taken at first clinical presentation. Note the large, well-defined radiolucency involving area of teeth #s 29-32. Also note a small and round radiolucency distal and inferior to the large lesion and below the inferior alveolar canal.
The patient’s past medical history is negative for any significant disease or risk factors.
The patient reported progressive swelling of the right posterior mandible of unknown duration. Teeth #s 29-31 were not mobile or painful. The swelling had perforated the buccal plate and there was no lingual bone per cone beam CT images. There were no other radiolucencies in the jaw bone other than a small lesion distal and inferior to the large lesion.
Treatment
Under local anesthesia, a full-thickness flap around area of teeth #s 30 & 31 was raised and an incisional biopsy was performed. The tissue was fleshy and vascular. The area was sutured and the specimen submitted for microscopic evaluation.
Excisional Biopsy
Histologic examination reveals multiple pieces of soft tissue composed of connective tissue with sheets of plasma cells intermixed with scattered small lymphocytes. The plasma cells were fairly uniform in appearance with scattered nucleoli present (Figure 2). Occasional Dutcher bodies were seen overlying the plasma cell nuclei. The plasma cell infiltrate was uniformly positive for CD138 (Figure 3) and kappa light chain (Figure 4) and negative for lambda light chain. Rare CD3+ T-cells were present. No immunoreactivity for CD20 was seen on the plasma cells; however, rare CD20+ cells were present.
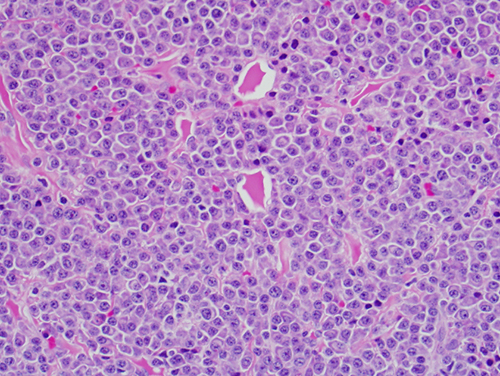
Figure 2. High power (x400) H & E histology shows sheets of plasma cells intermixed with scattered small lymphocytes. The plasma cells are fairly uniform in appearance.
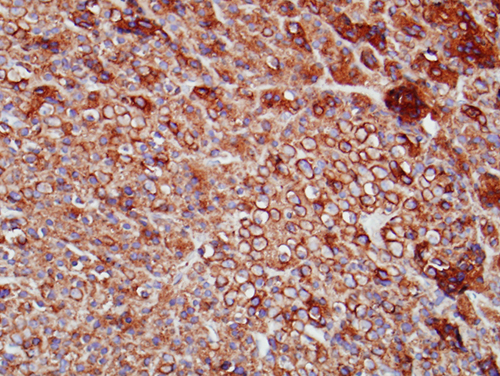
Figure 3. High power (x400) immunohistochemistry for CD138. Note uniformly positive staining with CD138, a marker for plasmacytoid cells.
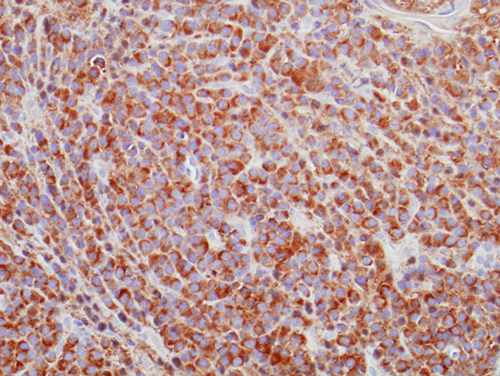
Figure 4. High power (x400) immunohistochemistry for kappa. Note uniformly positive staining with kappa light chain.
After you have finished reviewing the available diagnostic information