Return to Case of the Month Archives
May 2010: Large swelling; left posterior hard and soft palate
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Jim Reed
Eastside Oral & Maxillofacial Surgery
Bellevue, WA
Case Summary and Diagnostic Information

This is a 69-year-old gentleman referred by Medical Teams International for evaluation of a large left maxillary mass (Figure 1).
Diagnostic Information Available
This is a 69-year-old gentleman referred by Medical Teams International for evaluation of a large left maxillary mass (Figure 1). He reports that the lesion has been present for eight to ten years and occurred just after removal of tooth #16. The lesion has been slowly growing. It is not painful and it does not bleed.
Figure 1 This is a clinical photograph taken at the first clinical presentation; note the large exophytic and smooth-surfaced nodule in the left posterior hard palate and soft palate area. Also note the swelling behind the large nodule on the hard palate which is more diffuse.
His past medical history is significant for a vascular malformation of the right neck which extends through to the lateral pharynx, palate and maxilla diagnosed in 1958. This condition was treated in Ethiopia in 1963 with external beam radiation. He has otherwise been healthy.
At presentation, the patient’s chief complaint was a large mass in the posterior maxilla which was not painful. The mass was well-demarcated and the same color as the surrounding mucosa; it was exophytic and sessile with a smooth surface (Figure 1). It measured 3 x 2 x 0.5 cm and was not otherwise symptomatic. The palatal mucosa/gingiva located mesial to this obvious mass was also sessile and exophytic but more diffuse in appearance. The larger lesion was rubbery in consistency while the smaller lesion was less firm in consistency.
Figure 1 This is a clinical photograph taken at the first clinical presentation; note the large exophytic and smooth-surfaced nodule in the left posterior hard palate and soft palate area. Also note the swelling behind the large nodule on the hard palate which is more diffuse.
Treatment
The large mass and the lesion mesial to it were removed under general and local anesthesia. Aspiration yielded no blood. The mass was homogeneous, firm and rubbery in consistency. The mesial portion was less firm but also homogeneous. Specimens 1.0 x 0.8 cm and 0.8 x 0.5 cm respectively were removed. No unusual bleeding was encountered. Hemostasis was achieved with electrocautery. Specimens were sent in formalin for histologic examination.
Incisional Biopsy
Histologic examination reveals two multisected pieces of soft tissue composed of surface epithelium with underlying fibrous connective tissue infiltrated by a neoplasm of salivary gland origin (Figure 2). This neoplasm is infiltrative and is made up of uniform, small and basaloid epithelial cells some arranged in tubules (Figure 3), others in duct-like structures while others in islands with cribriform pattern (Figures 3 & 4). Occasional mitotic figures are present. There is no evidence of significant cellular atypia or pleomorphism.
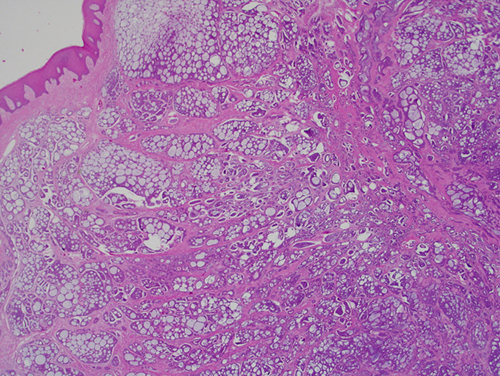
Figure 2 Low power (x40) H & E histology demonstrates a piece of mucosa infiltrated by many small, uniform basaloid cells some forming duct-like structures, others arranged in tubules while many others are arranged in islands with a cribriform pattern.
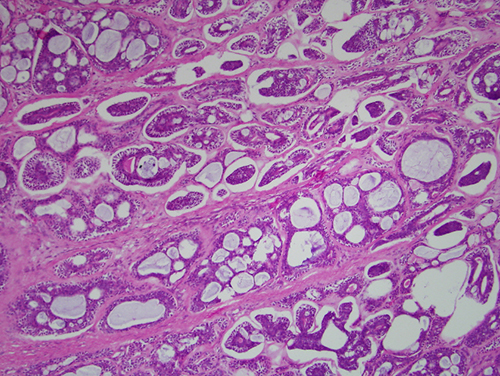
Figure 3 Higher power (x100) H & E histology demonstrates a closer look at the infiltrative neoplastic cells forming tubules and islands with a cribriform pattern.
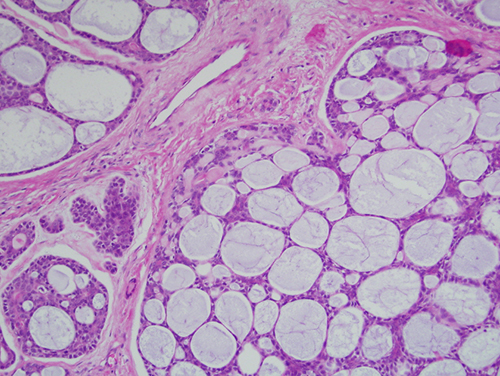
Figure 4 Higher power (x200) H & E histology demonstrates a higher magnification of the epithelial islands with a cribriform pattern.
After you have finished reviewing the available diagnostic information