Return to Case of the Month Archives
Well-defined and large radiolucency left ramus and condyle
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Jenette Intrachat, Jarom Luu & Ross Beirne
Seattle Indian Health Board and UW Dental School, Washington
Case Summary and Diagnostic Information
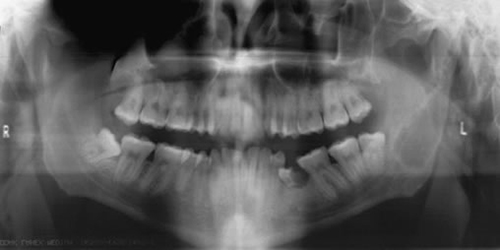
This is a 22-year-old Alaska Native male with history of 120 pounds of weight loss. He presented to Seattle Indian Health Board clinic for a routine dental visit. The head and neck examination was within normal limits. There is was no evidence of facial swelling or asymmetry or bony expansion. However, the panoramic radiograph (Figure 1) revealed a large, well-defined and corticated unilocular radiolucency of the left ramus extending and involving the condylar process and condylar head. The radiolucency of the condyle is multilocular.
Diagnostic Information Available
This is a 22-year-old Alaska Native male with history of 120 pounds of weight loss.
He presented to Seattle Indian Health Board clinic for a routine dental visit. The head and neck examination was within normal limits. There is was no evidence of facial swelling or asymmetry or bony expansion. However, the panoramic radiograph (Figure 1) revealed a large, well-defined and corticated unilocular radiolucency of the left ramus extending and involving the condylar process and condylar head. The radiolucency of the condyle is multilocular.
Figure 1 Panoramic view at first presentation demonstrating large unilocular radiolucency with corticated border involving most of the ramus and an extension multilocular radiolucency of the condyle.
This patient has a history of weight loss, having lost 120 pounds. In addition, he reports a history of multiple episodes of trauma (hits) to his face. His past medical history is also significant for acid reflux, cigarette smoking (quit in December 2007) and high blood pressure. The latter was the case when he was overweight; since his weight loss, his blood pressure has been within the normal range.
The panoramic radiograph demonstrates a well-defined and corticated unilocular radiolucent lesion occupying a significant portion of the left mandibular ramus extending superiorly into the condylar process and head. The radiolucency in the condylar head is multilocular. Cone beam CT read by Dr. lars Hollender demonstrated moderate expansion and thinning of the lingual/posterior aspects of the ramus (Figure 2) but there was no evidence of bone perforation. Other incidental radiographic findings include mucosal swelling of the right maxillary sinus, nasal septum deviation and supraeruption of tooth #1. Clinically and radiographically demonstrated retained tooth # L which was extracted.
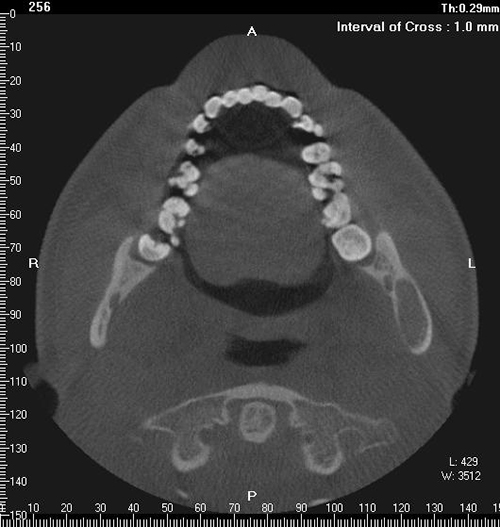
Figure 2 Cone Beam CT view demonstrating moderate expansion and thinning of the lingual bone. There was no evidence of bony perforation.
Treatment
Under IV sedation and in a transoral approach along the lateral left mandible, the area was subperiosteally dissected to the inferior border of the mandibular ramus. The lateral cortex bone was removed where dense fibrous tissue with a gritty consistency was encounter. There was no evidence of a bony cavity; the area was filled with solid material. Small fragments of this tissue were removed and submitted for histological evaluation. The surgical area was thoroughly irrigated and the soft sutured with 3.0 chromic gut suture. The patient was placed on Vicodin and a week of amoxicillin. At two week follow-up, patient complained of moderate discomfort. The area was healing well and the patient was placed on three-month follow up visit for repeat CT and panoramic radiographs.
Incisional and excisional biopsy
The incisional biopsy demonstrated multiple fragments of decalcified hard and soft tissue made up of a benign fibro-osseous (figures 3 & 4). It is composed of irregularly shaped woven-type bony trabeculae surrounded by slightly cellular fibrous connective tissue stroma. The bony trabeculae are of variable shapes and sizes, some are curvilinear. They show very little osteoblastic rimming. In focal areas, the connective tissue stroma is artifactually mildly retracted from the bony trabeculae (Figure 4).
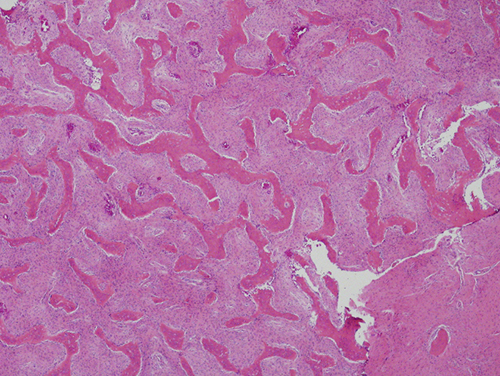
Figure 3 Low power (x100) histology shows a benign fibro-osseous type lesion with small and irregular bony trabeculae, some with curvilinear morphology. The connective tissue stroma is moderately cellular.
Figure 4 Higher power (x200) histology shows the irregular shaped bony trabeculae lacking osteoblastic rimming and directly lined by fibroblasts of the surrounding connective tissue stroma. Note the slight retraction of the connective tissue from the bony trabeculae.
After you have finished reviewing the available diagnostic information