Return to Case of the Month Archives
Lobular Exophytic Gingival Swelling
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Gretchen S. Folk, LCDR, DC, USNR
Naval Medical Center San Diego
Case Summary and Diagnostic Information

This is a 31-year-old male with an 11-month history of a sessile, lobular, progressively enlarging lesion in the anterior facial maxillary gingiva with palatal expansion.
Diagnostic Information Available
This is a 31-year-old male with an 11-month history of a sessile, lobular, progressively enlarging lesion in the anterior facial maxillary gingiva (Fig 1) with palatal expansion. Non-surgical root canal therapy was performed on teeth #s 9 & 10 in January 2004. The panoramic radiograph demonstrates slight divergence involving teeth #s 10 & 11 with minimal increased bone density (Fig 2). The preoperative blood cell counts were as follows: WBC 5.3, RBC 4.92, HGB 15.0, and PLT 186.
Figure 1. This is a clinical view of the lesion at presentation demonstrating multiple lobules of exophytic lesions on the facial maxillary gingiva, one appears to be ulcerating.

Figure 2. This is a panoramic radiograph demonstrating slight divergence of teeth #s 10 & 11 with increased bone density.
The patient describes a history of trauma to the area during childhood. The patient has no history of increased risk factors such as tobacco and alcohol use.
The hard tissue lesion is present mostly on the facial gingiva of the anterior maxilla. Slight expansion is also present on the palatal gingiva. Non-surgical root canal therapy was performed on teeth #s 9 & 10 in January 2004. The panoramic radiograph (Fig. 2) demonstrates slight divergence of teeth #s 10 & 11 with increased bone density in the same area. CT studies show an irregular sclerotic density extending from the maxillary left incisors to the left 1st premolar. The radiographic borders are ill-defined and irregular. The radiologist’s CT interpretation is osteomyelitis.
Figure 2. This is a panoramic radiograph demonstrating slight divergence of teeth #s 10 & 11 with increased bone density.
The incisional biopsy (Fig. 4) demonstrated malignant osteoid partially rimming lobules and sheets of malignant cartilaginous matrix. The hard tissue is surrounded and suspended by a fine network of malignant spindle-shaped cells with hyperchromatic and angular nuclei displaying a high degree of pleomorphism (Fig 5).
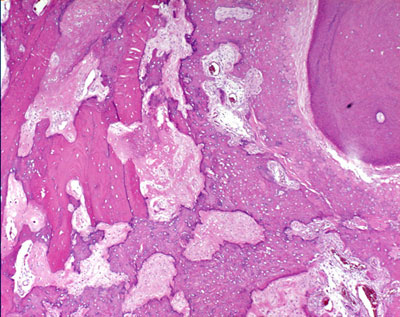
Figure 4. Low power (x200) histology illustrates malignant osteoid partially rimming lobules and sheets of malignant cartilaginous matrix. The hard tissue is suspended on a fine network of malignant spindle-shaped cells. Also present are lamellar bone and a fragment of tooth mostly in form of cellular and acellular cementum.
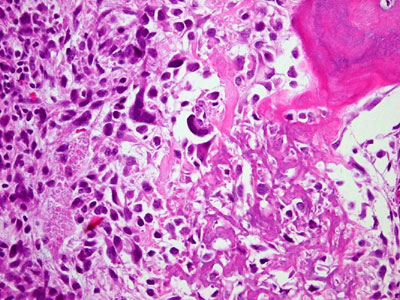
Figure 5. High power (x400) histology illustrates malignant cells with marked pleomorphism and anaplasia and malignant osteoid matrix. Also present is a fragment of tooth in form of cementum.
After you have finished reviewing the available diagnostic information