Return to Case of the Month Archives
Multilocular Radiolucency; Left Posterior Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. Anoosh Afifi & Thomas Hohl
General Dentistry and Oral & Maxillofacial Surgery, Seattle, WA
Case Summary and Diagnostic Information

This is a 44-year-old female who was seen by her general dentist on July 16, 2010 and was referred because of a radiolucent lesion noted on the panoramic radiograph.
Diagnostic Information Available
This is a 44-year-old female who was seen by her general dentist on July 16, 2010 and was referred because of a radiolucent lesion noted on the panoramic radiograph. Teeth #s19-22 tested vital. This radiolucent area was approximately 2 x 2 cm in size and was located in the mandibular body, below teeth #s18, 19 and 20. There was a slight swelling over the buccal of teeth #s18, 19, and 20. The patient had no pain or any other symptoms. Her past medical history is otherwise unremarkable.
Figure 1 Photograph taken in July 2010 represents the corticated and multilocular radiolucency in the left posterior mandible between teeth #s 18 and 20.
The patient’s past medical history is negative for any significant disease or risk factors.
This lesion was discovered during a routine panoramic radiograph taken in July 2010. The duration of the lesion is unknown. The lesion was slightly expansile on the buccal aspect but was otherwise not symptomatic. The associated teeth were vital. There was no evidence of tooth displacement or resorption.
Treatment
Under local anesthesia, an incisional biopsy was performed. The procedure involved laying a buccal flap in the area of teeth #s 18-21. Upon laying a flap, perforation of the buccal cortex was noted and the inferior alveolar nerve had been pushed buccally making it difficult to aggressively remove the mass. Small tissue samples were removed and submitted for microscopic evaluation. There was very little bleeding. Post operatively, the patient did well but has mild parasthesia of the lower lip and chin believed to be due to the nerve being pushed buccally. The patient is currently kept on recall visits to closely monitor any changes.
Incisional Biopsy
This biopsy was read by Dr. Thomas Morton, Oral Pathology Biopsy Service, School of Dentistry, University of Washington. Histologic examination reveals multiple pieces of soft tissue composed of loose and myxoid connective tissue containing a lesion of vascular origin. The latter is made up of vascular spaces of variable shapes and sizes lined by one layer of flat endothelial cells and separated by loose connective tissue.
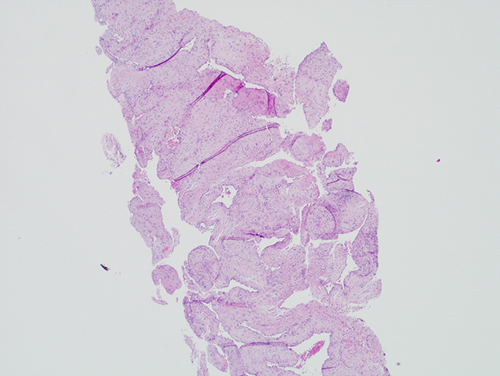
Figure 2 Low power (x40) H & E histology demonstrates loose and myxoid connective tissue with a lesion of vascular origin. The latter is made up of vascular spaces of variable shapes and sizes lined by one layer of flat endothelial cells and separated by loose connective tissue.
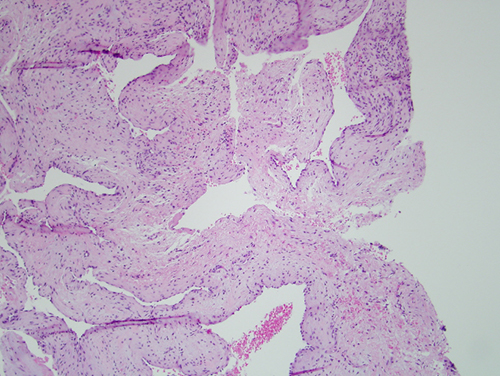
Figure 3 Low power (x100) H & E histology demonstrates vascular spaces of variable shapes and sizes separated by connective tissue and lined by one layer of flat endothelial cells.
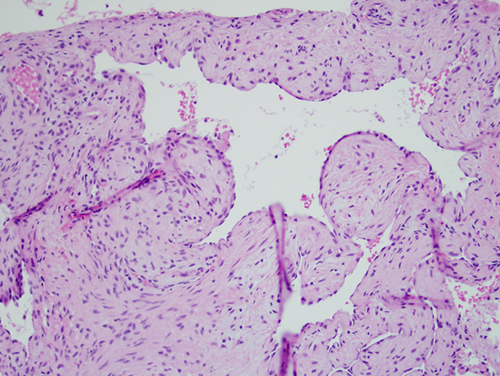
Figure 4 Low power (x100) H & E histology demonstrates vascular spaces of variable shapes and sizes separated by connective tissue and lined by one layer of flat endothelial cells.
After you have finished reviewing the available diagnostic information