Return to Case of the Month Archives
Unilocular Radiolucency Associated with an Impacted Third Molar
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. Ilana Kaplan, Shlomo Calderon
Institute of Pathology and Oral & Maxillofacial Surgery, Israel
Case Summary and Diagnostic Information

This is a 47-year-old male with an incidental discovery of a left mandibular radiolucency around an impacted tooth #17.
Diagnostic Information Available
This is a 47-year-old male with an incidental discovery of a left mandibular radiolucency around an impacted tooth #17. The area was asymptomatic with no evidence of swelling, expansion or pain. Although the lesion extended inferiorly and pushed on the alveolar canal (Fig 1), no neural deficit was detected. Patient has a history of tobacco use. He ceased smoking a year ago. The pre-operative WBC was 7.5, RBC 4.9, HGB 15.7 and PLT 298.
Figure 1. Panoramic view at first presentation demonstrating a well-demarcated, unilocular radiolucency extending posteriorly into the ramus and associated with the crown of an impacted third molar.
There was no relevant medical history to this lesion; and there is no family history of related disease. The patient had a history of depressive disorder but has been off the medications for at least two years. His oral hygiene was reasonably good, dental and periodontal conditions were rendered as good.
The patient presented for a routine dental cleaning when this lesion was discovered as an incidental finding. The patient has all his four third molars, one erupted (tooth #1) and three impacted (teeth #s 16, 17 and 32). He also has multiple endodontically treated teeth and one four unit bridge in the posterior maxilla (Fig 1). Tooth # 17 shows a large, unilocular radiolucency with smooth and corticated borders pushing on the inferior alveolar canal and growing posteriorly into the ramus. The radiolucency surrounds the crown of tooth # 17 from the cemento-enamel-junction (CEJ) to CEJ. Despite the size of this lesion, there was no clinical evidence of significant expansion.
Figure 1. Panoramic view at first presentation demonstrating a well-demarcated, unilocular radiolucency extending posteriorly into the ramus and associated with the crown of an impacted third molar.
Histologic examination revealed a cystic structure with lining epithelium and a supporting fibrous connective tissue wall (Fig 2 & 2a). The latter is focally myxoid with occasional to no inflammatory cells and dilated small blood vessels. The histologic features of the lining epithelium of this cyst are as follow: the epithelium is of variable thickness and is stratified squamous in type. It is interspersed with spaces (microcysts or duct-like spaces without the cuboidal cells lining the spaces). The epithelium is superficially lined by one layer of cuboidal cells interspersed with mucous producing cells (Fig 3) as demonstrated by the special stain (Alcian blue) staining mucous bright blue.
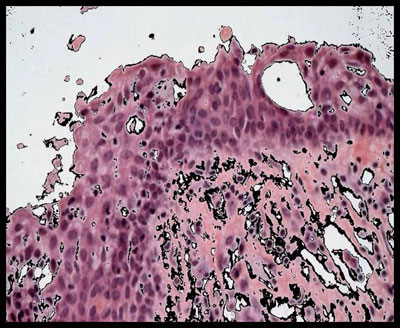
Figure 2 & 2a. 10x magnification demonstrating a cystic structure with lining epithelium and a supporting fibrous connective tissue wall (Fig 2 & 2a). The lining epithelium is stratified squamous in type interspersed with spaces (microcysts or duct-like spaces without the cuboidal cells lining the spaces). The epithelium is superficially lined by one layer of cuboidal cells interspersed with mucous producing cells.
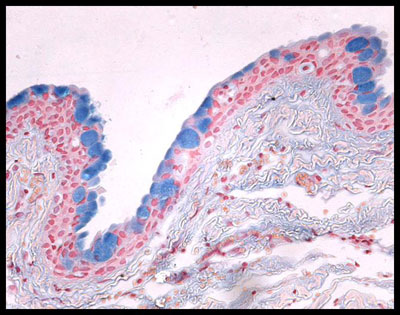
Figure 3. 10x magnification demonstrating positive staining for mucin within the spaces in the lining epithelium using Alcian blue special stain for mucin.
After you have finished reviewing the available diagnostic information