Return to Case of the Month Archives
Large exophytic swelling, right retromolar pad area and gingiva of tooth #31
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Brian Jackson
Oral & Maxillofacial Surgery, Olympia, WA
Case Summary and Diagnostic Information

This is a 61-year-old white female who had a slowly and progressively enlarging gingival swelling at right retromolar pad area, gingiva of tooth #31 and right posterior vestibule.
Diagnostic Information Available
This is a 61-year-old white female who had a slowly and progressively enlarging gingival swelling over the last six months (Figure 1 & 2). It involved the right retromolar pad area, the buccal gingiva of tooth #31 and the right posterior vestibule. The swelling was mostly in the right retromolar pad area (Figure 1). The patient complained of soreness in the area. It was pink to red in color and was focally ulcerated and lobular. It was described clinically to be around 2.5 cm in size. There was no evidence of underlying bone involvement (Figure 3). The patient’s past medical history is negative for smoking.
Figure 1. Photograph is taken at first clinical presentation demonstrating a large, sessile, exophytic, focally red and ulcerated swelling of the right posterior mandibular vestibule, buccal gingiva of tooth #31 and the right retromolar pad area.

Figure 2. Photograph is taken at first clinical presentation demonstrating a large, sessile, exophytic, focally red and ulcerated swelling mostly of the right retromolar pad area.

Figure 3. Panoramic view taken at first clinical presentation demonstrating normal bone and no evidence of tooth displacement or bone resorption in the right posterior mandible.
The patient’s past medical history is negative for smoking. Present medications are Lovastatin, calcium, and multivitamins. She has a history of pericarditis in 1977.
The patient reported a slowly enlarging pink-red, focally ulcerated and lobular swelling of the posterior vestibule, the buccal gingiva of tooth #31 and the right retromolar pad area (Figure 1 & 2). The lesion was of six months’ duration and was described as 2.5 cm in size. It was mildly painful and was progressively getting larger. There was no evidence of bone resorption or tooth displacement as demonstrated in (Figure 3).
Figure 1. Photograph is taken at first clinical presentation demonstrating a large, sessile, exophytic, focally red and ulcerated swelling of the right posterior mandibular vestibule, buccal gingiva of tooth #31 and the right retromolar pad area.
Figure 2. Photograph is taken at first clinical presentation demonstrating a large, sessile, exophytic, focally red and ulcerated swelling mostly of the right retromolar pad area.
Figure 3. Panoramic view taken at first clinical presentation demonstrating normal bone and no evidence of tooth displacement or bone resorption in the right posterior mandible.
Treatment
Under local anesthesia, an incisional biopsy was performed. After the histopathologic diagnosis, a complete surgical removal was performed under general anesthesia.
Incisional Biopsy
Histologic examination reveals multiple pieces of soft tissue composed of surface epithelium with underlying fibrous connective tissue almost all occupied by a neoplasm of salivary gland origin. This neoplasm is infiltrative and has no capsule and is made up of mucus-producing cells surrounded by epidermoid cells (Figure 4 & 5). It is arranged in duct-like structures with cystic degeneration in some areas and nests of cells in others (Figures 4 & 5). The lumen of the duct-like structures contains mucoid material as well as some macrophages and neutrophils. The connective tissue is loose and vascular in some areas and fibrotic in others. It is also infiltrated by many lymphocytes, plasma cells and neutrophils. Mucicarmine (Figure 6) and periodic acid Schiff stains are positive for mucin.
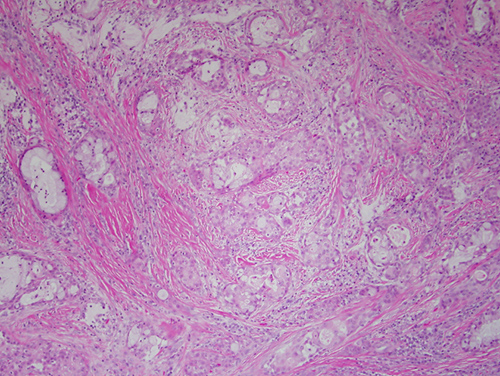
Figure 4. Low power (x100) the H & E histology reveals an infiltrative neoplasm made up of mucus producing cells surrounded by epidermoid cells. It is arranged in duct-like structures with cystic degeneration in some areas and nests of cells in others.
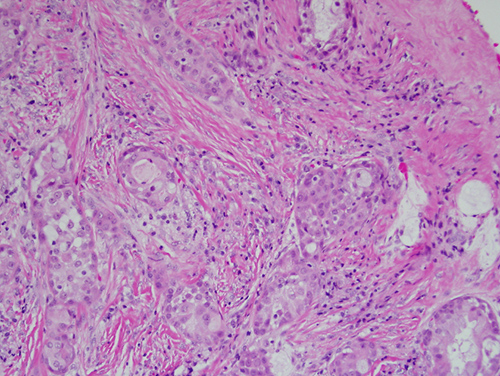
Figure 5. Higher power (x200) the H & E histology of a slightly higher power shows an infiltrative neoplasm with duct-like structure and small epithelial islands composed of epidermoid and mucous producing cells.
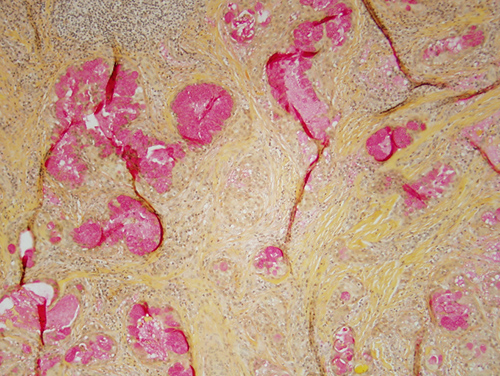
Figure 6. Low power (x100) Mucicarmine stain is positive for mucous producing cells present within the duct-like structure and epithelial islands comprising this infiltrative neoplasm.
After you have finished reviewing the available diagnostic information