Return to Case of the Month Archives
Mandibular Cyst
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Wesley L. Hanson, D.D.S., M.S.D., P.S.
Poulsbo Periodontics & Implant Center
Case Summary and Diagnostic Information
This is a 12-year-old healthy Caucasian male who presented at his General Dentist office for a routine dental examination, radiographs and dental prophylaxis.
Diagnostic Information Available
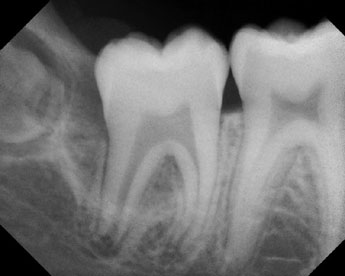
This is a 12-year-old healthy Caucasian male who presented at his General Dentist office for a routine dental examination, radiographs and dental prophylaxis on 04/2004. The Panoramic x-ray revealed a deep, radiolucent area of bone loss at the distal of tooth # 31 (Fig 1) that extended distally to the follicular sack surrounding the developing crown of tooth # 32. The asymptomatic, periodontal pocket measured 10 mm along the disto-buccal of tooth # 31, which prompted the dentist to refer the patient for periodontal evaluation and treatment.
Figure 1. A curved line along the buccal aspect of tooth #31 corresponding to the 10 + mm pocket clinically detected along the distobuccal aspect of this tooth.
Other than a routine appendectomy surgery on February 2004, the patient’s medical history was unremarkable. Both Vicodin and Morphine had been prescribed post-surgically but no medications were being taken at the time of the initial examination at the periodontist’s office on 05/2004. The dental history was also unremarkable. There is no family history of similar dental problems within either parent’s background.
The patient presented with a generally healthy dentition and average plaque control for a teenaged boy. The periodontal health was unremarkable except for a 10+ mm pocket located at the distobuccal of tooth #31, which was found to have subgingival inflammation and suppuration during probing. The contra-lateral tooth # 18 had a 5 – 6 mm probing depth with thickened retro-molar gingiva on the distal root surface. Radiographically, the lesion between teeth #’s 31 – 32 appears as a narrow, buccal curve along the tooth with an osseous defect, with the developing crown of tooth #32 lying superiorly and horizontally impacted. The lamina dura and the periodontal ligaments around teeth #’s 18 and 31 appear to be intact. No radiographic change was apparent around tooth #18 (Fig 2). Tooth # 31 is vital and responded so endodontically to the application of ice.

Figure 2. Although a 5-6 mm probing depth was detected at the buccal aspect of tooth #18, there are no radiographic changes to correspond to it.
The biopsy specimens showed fragments of loose and vascular granulation tissue covered by proliferative stratified squamous epithelium. The latter contained clusters of neutrophils (Fig 4). The granulation tissue supporting the epithelium was infiltrated by many neutrophils, lymphocytes, plasma cells and foamy macrophages (Fig 5)
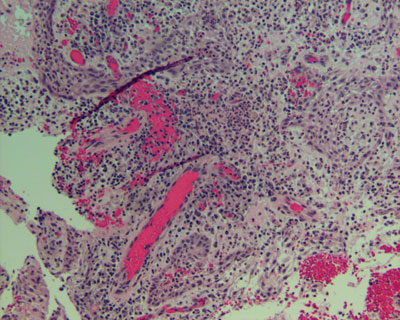
Figure 4. Low power (x200) histology shows small fragments of loose and vascular granulation tissue covered by non-keratinized and proliferative stratified squamous epithelium containing small clusters of neutrophils.
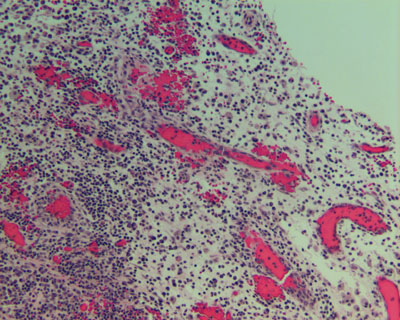
Figure 5. Low power (x200) Histology similar to Figure 4 demonstrating a supporting granulation tissue infiltrated by many acute and chronic inflammatory cells.
After you have finished reviewing the available diagnostic information