Return to Case of the Month Archives
April 2009: Large gingival swelling, left posterior mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. M DaBell and M Englestadt
Harborview Medical Center, Seattle WA
Case Summary and Diagnostic Information

This is an 83-year-old black female who presented to the emergency clinic at Harborview Medical Center with gingival swelling and pain in the left posterior mandibular alveolar ridge between teeth #s 18 and 20; tooth # 19 was missing (Figure 1). The patient stated that the area was painful, especially when biting down. The area had been sensitive for several weeks and had been swollen for a few months. The panoramic radiograph showed ill-defined radiolucency in the area of missing tooth #19 (Figure 2). The swelling measured 2 x 2 centimeters with 1.5-cm height. There was no history of tobacco or alcohol use.
Diagnostic Information Available
This is an 83-year-old black female who presented to the emergency clinic at Harborview Medical Center with gingival swelling and pain in the left posterior mandibular alveolar ridge between teeth #s 18 and 20; tooth # 19 was missing (Figure 1). The patient stated that the area was painful, especially when biting down. The area had been sensitive for several weeks and had been swollen for a few months. The panoramic radiograph showed ill-defined radiolucency in the area of missing tooth #19 (Figure 2). The swelling measured 2 x 2 centimeters with 1.5-cm height. There was no history of tobacco or alcohol use.
Figure 1 Photograph taken at first clinical presentation to Harborview Medical Center. Note the pink, sessile swelling between teeth #s 18 & 20. Tooth # 19 is missing. The mucosa is intact and shows no evidence of ulceration.
The patient’s past medical history is significant for congestive heart failure, hypertension, sick sinus syndrome and Glaucoma. Her medications included Lisinopril 15mg PO qday, ASA 81 mg po daily, Doxazosin 4mg PO qhs, Lasix 20mg PO daily, and Gabapentin 300mg po qhs prn.
The clinical presentation included a progressive swelling in the left posterior mandible, which became sensitive in the last few weeks and was painful at presentation. Pain increased with biting. The soft tissue swelling was pink and the overlying mucosa was intact with no evidence of ulceration (Figure 1). Radiographically, the area showed ill-defined radiolucency in the area of missing tooth #19 (Figure 2). It was an isolated lesion.
Figure 1 Photograph taken at first clinical presentation to Harborview Medical Center. Note the pink, sessile swelling between teeth #s 18 & 20. Tooth # 19 is missing. The mucosa is intact and shows no evidence of ulceration.

Figure 2 Panoramic radiograph demonstrating bone resorption, left posterior mandible in the area of teeth #s 18-20. This radiograph reveals an ill-defined radiolucency with reactive bone at the inferior margin.
Treatment
The lesion was biopsied under local anesthesia. The results of the incisional biopsy led to a referral to an oncologist for further treatment.
Incisional Biopsy
This case was diagnosed by Dr. Heike Deubner at Department of Pathology, Harborview Medical Center. We thank Dr. Deubner for the diagnosis and the histology photographs.
Histologic examination of the H & E section revealed sheets of small blue round cells representing atypical cells (Figure 3) which with higher magnification appeared to be atypical plasma cells with moderate nuclear pleomorphism, and prominent nucleoli (Figure 4). Mitotic figures were identified. Immunohistochemical stains were uniformly and strongly positive with CD138 and Kappa light chain and negative with Lambda light chain (Figure 5).
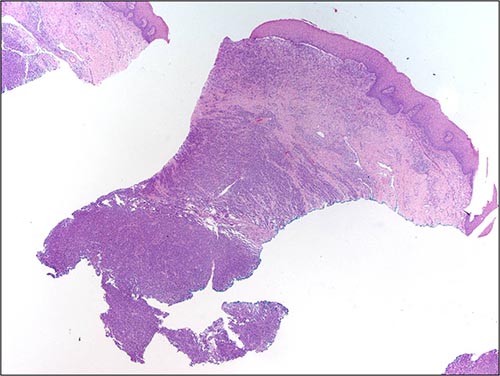
Figure 3 Low power (x40) H & E histology shows oral mucosa covered by epithelium and supported by connective tissue infiltrated by sheets of small round blue cells. The sheets of cells are denser at the bottom part of the connective tissue. We thank Dr. Deubner for the diagnosis and the histology photographs.
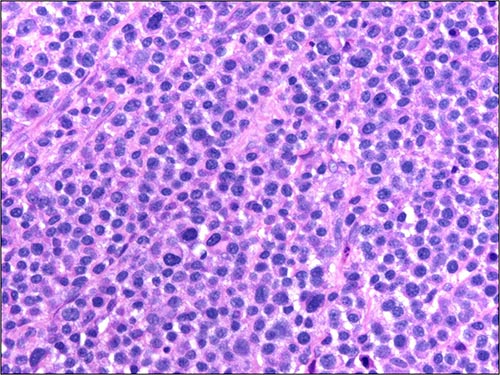
Figure 4 High power (x400) histology shows sheets of plasma cells, most are large and atypical with large nuclei and prominent nucleoli. Occasional normal and mature plasma cells are present. We thank Dr. Deubner for the diagnosis and the histology photographs.
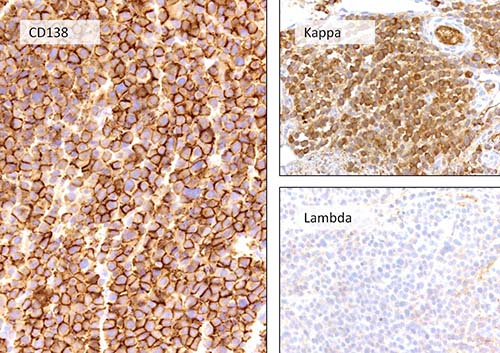
Figure 5 High power (x400) immunohistochemistry for kappa, lambda and CD138. Note uniform positive staining with kappa light chain but negative with lambda. It is also uniformly positive with CD138, a marker for plasmacytoid cells. We thank Dr. Deubner for the diagnosis and the histology photographs.
After you have finished reviewing the available diagnostic information