Return to Case of the Month Archives
Single deep ulcer lower lip
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Charles R. Weber
South Sound Oral Surgery, Olympia and Centralia, Washington
Case Summary and Diagnostic Information

This is a 64-year old white male who was referred with a two-year history of right lower lip lesion which was slowly enlarging. At presentation, this lesion was red and ulcerated (Figure 1) and was firm but not painful. It was 1.5 X 1.5 cm in greatest dimensions. The patient gives a 30 plus year history of smoking and indicates that “the ulcer is right where I hold my cigarette”. There was no evidence of lymphadenopathy. An incisional biopsy was performed and submitted for histologic evaluation.
Diagnostic Information Available
This is a 64-year old white male who was referred with a two-year history of right lower lip lesion which was slowly enlarging. At presentation, this lesion was red and ulcerated (Figure 1) and was firm but not painful. It was 1.5 X 1.5 cm in greatest dimensions. The patient gives a 30 plus year history of smoking and indicates that “the ulcer is right where I hold my cigarette”. There was no evidence of lymphadenopathy. An incisional biopsy was performed and submitted for histologic evaluation.
Figure 1 This clinical photograph represents the lesion at the first clinical presentation and before surgery. It is a non-healing, deep and rolled-bordered ulcer on the right side of the lower lip.
His past medical history is significant for 30 pack-years of smoking cigarettes. He admitted occasional alcohol use, drinking mainly beer and wine. His only other significant medical history is a seizure disorder well controlled with Dilantin.
The clinical examination revealed a 1.5 X 1.5 cm ulcerated red and white mass with rolled borders located on the right side of the lower lip near the commissure area (Figure 1). There were no palpable lymph nodes.
Figure 1 This clinical photograph represents the lesion at the first clinical presentation and before surgery. It is a non-healing, deep and rolled-bordered ulcer on the right side of the lower lip.
Treatment
Upon histologic confirmation of the diagnosis, referral was made to an otolaryngologist specializing in head and neck oncology for additional work-up and definitive treatment. Because of the size and duration of the lesion, both a wide local resection of the lower lip and a supra-omohyoid neck dissection was performed.
Incisional and excisional biopsy
Histological examination revealed a piece of oral mucosa exhibiting epithelial changes invading the underlying fibrous connective tissue. The epithelial cells show evidence of alteration in the nuclear/cytoplasmic ratio, loss of maturation, large nuclei with prominent nucleoli, increased mitotic activity and mild nuclear and cellular pleomorphism (Figure 2). Individual cell keratinization and keratin pearls are also present (Figure 3). Also present are clusters of foreign body type giant interpreted as foreign body reaction to keratin.
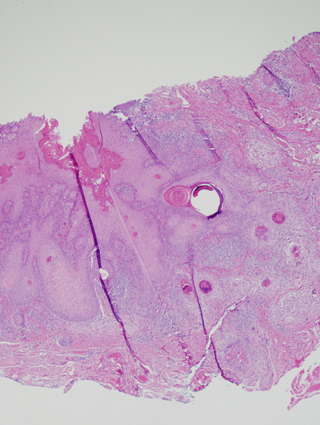
Figure 2 H & E stained section at screening 100X magnification demonstrating neoplastic epithelial cells invading the connective tissue in form of islands.
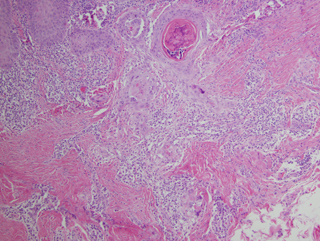
Figure 3 H & E stained section at 200x magnification demonstrating neoplastic epithelial islands with keratin pearl formation and cells with hyperchromatic nuclei and prominent nucleoli.
After you have finished reviewing the available diagnostic information