Return to Case of the Month Archives
An Ulceration of the Tongue
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Neal Futran, University of Washington, School of Medicine
Case Summary and Diagnostic Information
The clinical examination revealed a 3×5 cm ulcerated white mass on the right mid-lateral border of the tongue of a male patient.
Diagnostic Information Available
This is a 46-year old white male who presented at the University of Washington otolaryngology clinic with a 4-5 month history of a painful, slowly enlarging “sore” on the right lateral border of the tongue. At presentation he required Oxycodone medication for pain control.
The patient had increased difficulty swallowing and as a result had lost 5 pounds in 6 weeks. He had no airway problems and neck examination was negative for any masses. He has a 30-pack per year history of smoking cigarettes and currently smokes 10 cigarettes per day. He drank 1 quart of alcohol per week in his 30’s, but now only has 1-2 alcoholic drinks per week. He has no history of alcohol withdrawal and he has no chemical exposure. His past medical history and past surgical history are otherwise unremarkable.
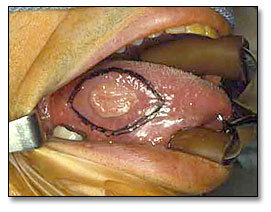
The clinical examination revealed a 3×5 cm ulcerated white mass on the right mid-lateral border of the tongue that was not adherent to the mandibular alveolar ridge. The ulcer had rolled borders (Figure 1). There were no palpable lymph nodes. He was staged T3N0M0.
Figure 1. This clinical photograph represents the lesion before surgery. White, non-healing rolled-bordered ulcer on the mid lateral border of Tongue.
Histological examination revealed a piece of oral mucosa exhibiting epithelial changes
invading the underlying fibrous connective tissue, superficial skeletal muscle bundle and salivary gland lobules. The epithelial cells show evidence of alteration in the nuclear/cytoplasmic ratio, loss of maturation, increased mitotic activity and mild nuclear and cellular pleomorphism (Figure 4). Individual cell keratinization and keratin pearls are also present (Figure 5).
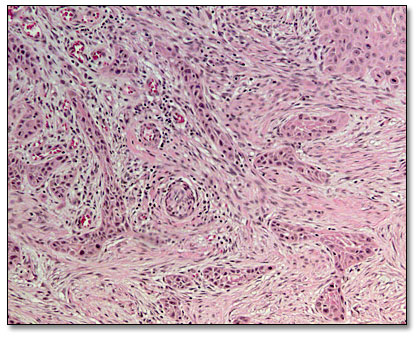
Figure 4. H & E stained section at 40X magnification demonstrating neoplastic epithelial cells of variable sizes invading the connective tissue.
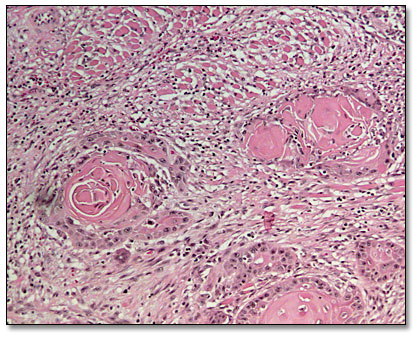
Figure 5. H & E stained section at 100x magnification demonstrating neoplastic epithelial islands with keratin pearl formation and cells with hyperchromatic nuclei and prominent nucleoli.
After you have finished reviewing the available diagnostic information