Return to Case of the Month Archives
Diffuse and Deep Ulceration
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Drs. David Molen & Namou Kim
Auburn Oral & Maxillofacial Surgery and Swedish Hospital Otolaryngology Department
Case Summary and Diagnostic Information

This is a 32-year old white female who presented at the Auburn Oral & Maxillofacial Surgery Clinic with a 3-month history of a painful, slowly enlarging “ulcer” on the left ventral/lateral border of the tongue.
Diagnostic Information Available
This is a 32-year old white female who presented at the Auburn Oral & Maxillofacial Surgery Clinic with a 3-month history of a painful, slowly enlarging “ulcer” on the left ventral/lateral border of the tongue (Figure 1) for which she was taking Vicodin. The lesion was described as 2 x 4 cm in size, reddish-white, and ulcerated. The patient reported pain on swallowing and was beginning to have difficulty swallowing solid foods, which prompted her presentation. There were no palpable cervical lymph nodes noted by either of the two surgeons. The CT scan however, revealed one irregular-appearing level IIA lymph node, 1.7cm in diameter.
Figure 1. This photograph represents the lesion at first clinical presentation and before surgery. Note the diffuse deep ulcers on the left lateral and ventral tongue with focally rolled bordered.
Her past medical history is significant for a recent sinus infection and gall bladder removal in August 2010. She reports cigarette smoking (½ ppd for 14 years) and is a social drinker. She is otherwise healthy.
The clinical examination revealed a 2×4 cm ulcerated white to red deep lesion on the left tongue involving most of the ventral tongue (Figure 1). The ulcer was deep and painful and was of three months’ duration. The ulcerated surface was flat in some areas and had rolled borders in others (Figure 1). There were no palpable lymph nodes at the first presentation.
Figure 1. This photograph represents the lesion at first clinical presentation and before surgery. Note the diffuse deep ulcers on the left lateral and ventral tongue with focally rolled bordered.
Treatment
Under local anesthesia an incisional biopsy was performed. Based on the diagnosis of the incisional biopsy, the patient underwent left partial glossectomy and left comprehensive neck dissection.
Incisional and Excisional Biopsy
Histologic examination reveals multiple pieces of soft tissue composed of surface epithelium exhibiting neoplastic changes invading the underlying fibrous connective tissue (Figure 2). The surface epithelium shows evidence of neoplastic changes; some confined to the surface while most others invading the connective tissue. The invasion is also in form of sheets as well as nests of neoplastic cells. The neoplastic cells show evidence of alteration in the nuclear/cytoplasmic ratio, loss of maturation, cells with large nuclei and prominent nucleoli, nuclear and cellular pleomorphism, individual cell keratinization and a few keratin pearls. Some of the neoplastic cells invaded the underlying skeletal muscle bundles (Figure 3). Immunohistochemistry for p16 was performed and was strongly positive (Figure 4).
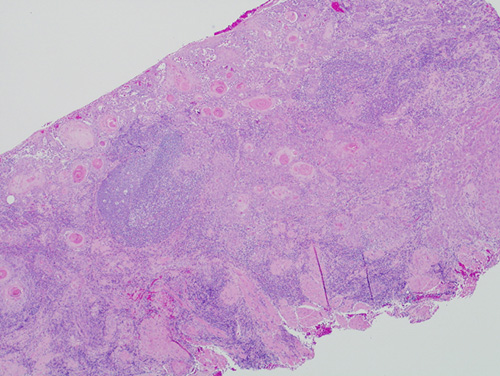
Figure 2. Low power (x100) H & E histology demonstrating neoplastic epithelial islands, of variable shapes and sizes, invading the connective tissue.
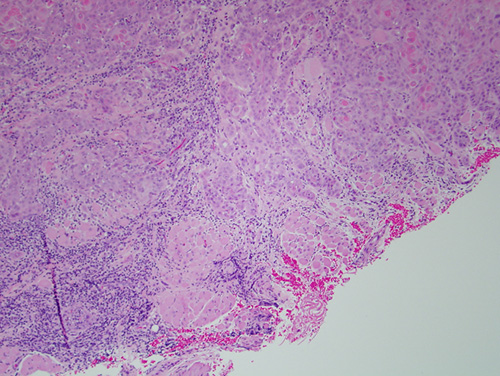
Figure 3. Higher power (x200) H & E histology demonstrating neoplastic epithelial islands deep within the connective tissue and invading the underlying skeletal muscle bundles.
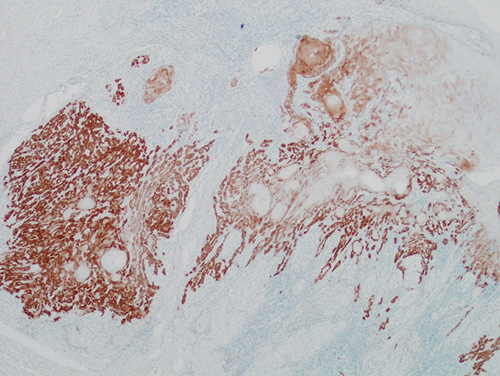
Figure 4. Higher power (x200) Immunohistochemistry staining with p16 demonstrating strongly positive staining of the neoplastic epithelial islands invading the connective tissue.
After you have finished reviewing the available diagnostic information