Return to Case of the Month Archives
September 2009: Large gingival swelling lingual right posterior mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Antonio Caso
Oral & Maxillofacial Surgery, Walla Walla, WA
Case Summary and Diagnostic Information

This is a 57-year-old white male with a slowly and progressively enlarging gingival swelling lingual of teeth #s 29-30 and the posterior edentulous mandible.
Diagnostic Information Available
This is a 57-year-old white male with a slowly and progressively enlarging gingival swelling lingual of teeth #s 29-30 and the posterior edentulous mandible. A similar, but smaller lesion was removed six years ago from the same area. This swelling is of one and a half years’ duration and has been growing slowly. It is reddish-purple in color and is ulcerated but not painful. The patient frequently bites the lesion as it interferes with chewing. It is described clinically to be hemorrhagic (bleeds easily), fungating and in excess of 2.5 x 3.5 cm in size. Tooth #30 is significantly displaced and the edentulous alveolar ridge is superficially resorbed, leading to the so-called “saucerization” of the alveolar bone (Figure 2).
Figure 1 Photograph is taken at clinical presentation demonstrating a large, exophytic, reddish gingival mass on the lingual area of teeth #s 29 & 30 and extending posteriorly to involve the edentulous alveolar ridge.
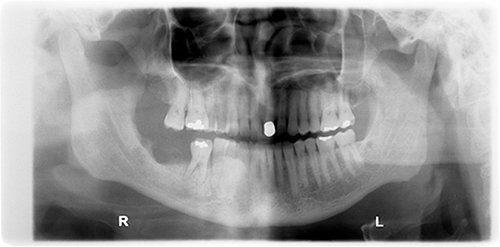
Figure 2 Panoramic radiograph taken at clinical presentation. It shows superficial and smooth-bordered resorption of the edentulous alveolar ridge.
The patient’s past medical history is significant for smokeless tobacco use for 17 years; he continues his tobacco use to the present. He also has a history of right-lobe thyroid tumor which was successfully treated with surgical resection.
The patient reported a slowly enlarging red-purple swelling lingual of the posterior mandible of one and a half years’ duration (Figure 1). A similar, smaller swelling was removed six years ago from the same location. The swelling was described as ulcerated and fungating but was not painful. The swelling had displaced tooth #30 almost completely outside the dentoalveolar housing. The first biopsy was performed in February and the lesion was completely removed in March. The incisional biopsy taken in February measured 1.2 x 1.0 x 0.4 cm while the complete surgical specimen arrived in two sections measuring 3.5 x 3.6 x 2.0 and 2.1 x 0.7 and 0.3 cm at its greatest dimensions. A panoramic radiograph shows that the alveolar ridge is superficially resorbed, leading to the so called “saucerization” of the alveolar bone (Figure 2).
Figure 1 Photograph is taken at clinical presentation demonstrating a large, exophytic, reddish gingival mass on the lingual area of teeth #s 29 & 30 and extending posteriorly to involve the edentulous alveolar ridge.
Figure 2 Panoramic radiograph taken at clinical presentation. It shows superficial and smooth-bordered resorption of the edentulous alveolar ridge.
Treatment
Under local anesthesia, an incisional biopsy was performed. After histopathologic review verified the diagnosis, a complete surgical removal was performed under local anesthesia per the patient’s request. Tooth #30 was extracted at the time of surgical resection and resection of the tumor was performed with a combination of blunt and sharp dissection and the use of a laser. Due to the extension of the tumor into the lingual mandible, care was taken to preserve the lingual nerve. The underlying mandibular bone was curetted with rotary instrumentation and copious irrigation. Local flaps were then advanced for soft tissue closure. The patient was referred to his primary care physician for evaluation for hyperparathyroidism. Lab results were all within normal limits and included a Parathyroid Hormone Intact Molecule of 35 pg/ml (normal: 12 – 88).
Incisional Biopsy
Histologic examination of the H & E sections from both the incisional specimen and the surgical specimens were similar in morphology. They were made up of mostly ulcerated surface epithelium with underlying cellular and vascular granulation tissue (Figure 3) containing numerous giant cells (Figures 4 & 5). The giant cells were of variable shapes and sizes haphazardly arranged. Clusters of hemosiderin pigment were present, especially in the superficial lamina propria (Figures 4 & 5). Also present were clusters of extravasated erythrocytes scattered throughout the granulation tissue stroma (Figures 4 & 5).
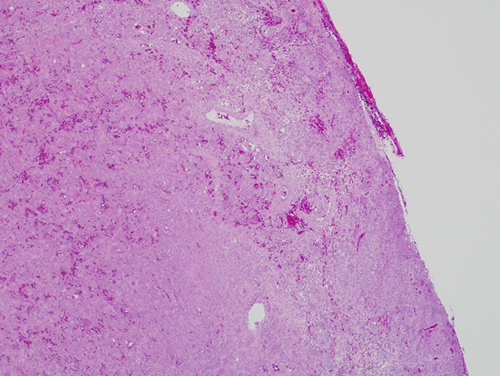
Figure 3 Low power (x40) the H & E histology reveals a mass of vascular and cellular granulation with ulcerated surface epithelium.
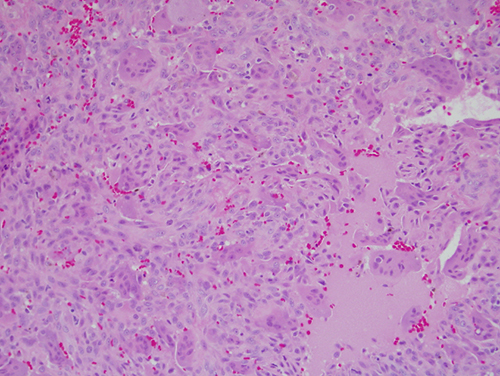
Figure 4 Low power (x100) the H & E histology of a slightly higher power shows the granulation tissue to contain numerous giant cells of variable shapes and sizes. Also present are clusters of extravasated erythrocytes and small clusters of hemosiderin pigment.
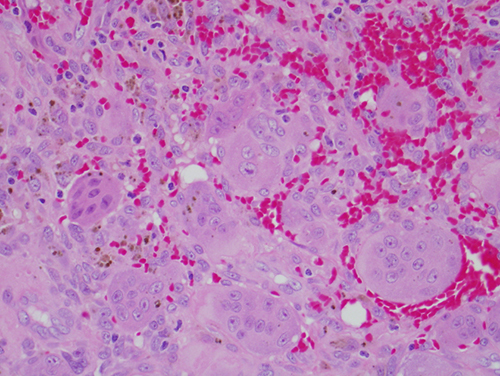
Figure 5 High power (x400) the H & E histology shows vascular granulation tissue with numerous giant cells, hemosiderin pigment and clusters of extravasated erythrocytes.
After you have finished reviewing the available diagnostic information