Return to Case of the Month Archives
Well-demarcated radiolucency, Anterior Mandible
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Michael Medley
Oral & Maxillofacial Surgery, Olympia, WA
Case Summary and Diagnostic Information

This is a 26-year-old female with some swelling and radiolucency of the anterior mandible of approximately four years’ duration.
Diagnostic Information Available
This is a 26-year-old female with some swelling and radiolucency of the anterior mandible (Figure 1) of approximately four years’ duration. The swelling is described to be four cm in size and causing slight tooth mobility. The patient complained of mild pain, especially with movement of the incisor teeth. There was no paresthesia. One month prior to this presentation, tooth #24 was endodontically treated and was found to be non-vital by the referring dentist. Clinical examination revealed slight expansion of the anterior buccal and lingual vestibules. With the exception of tooth #24, all of the anterior teeth tested vital. A sectional CT showed some expansion of the anterior mandible with significant thinning of the cortices, especially on the lingual aspect where there were areas in which the cortex could not be visualized.
Figure 1. This radiograph was taken in first clinical presentation. Note the relatively well-demarcated and partially corticated radiolucency anterior mandible. It is in the vicinity of the endodontically treated tooth #24.
The patient’s past medical history is positive only for treatment of anxiety and acne.
The patient reported progressive swelling of the anterior mandible (Figure 1) of four years’ duration. Clinical examination revealed slight expansion of the anterior buccal and lingual vestibules. With the exception of tooth #24, all of the anterior teeth tested vital. A sectional CT showed some expansion of the anterior mandible with significant thinning of the cortices, especially on the lingual aspect where there were areas in which the cortex could not be visualized.
Figure 1. This radiograph was taken in first clinical presentation. Note the relatively well-demarcated and partially corticated radiolucency anterior mandible. It is in the vicinity of the endodontically treated tooth #24.
Treatment
Aspiration of the lesion was negative. Under intravenous anesthetic a vestibular incision was made over an intact buccal cortex. Bone was removed to reveal a solid growth that was friable and hemorrhagic. The lesion was thoroughly curetted. Significant bleeding was encountered from vessels which were tied off. The lingual cortex was noted to be partially missing.
Excisional Biopsy
Histologic examination reveals multiple pieces of decalcified hard and soft tissue composed of a fibro-osseous lesion (Figure 2) with small clusters of giant cells. The fibro-osseous lesion is made up of cellular fibrous connective tissue stroma intermixed with calcified material, mostly young bone with a feathery appearance (Figure 3). The cellular connective tissue stroma is made up of spindle-shaped cells arranged in short bundles crisscrossing each other in some areas and arranged in a haphazard manner in others. Occasional mitotic figures are identified but the cells show no evidence of atypia. The spindle-shaped cells surround bony trabeculae and calcified material with a feathery consistency arranged in clusters surrounded by the soft tissue stroma. Also present are small clusters of multinucleated giant cells.
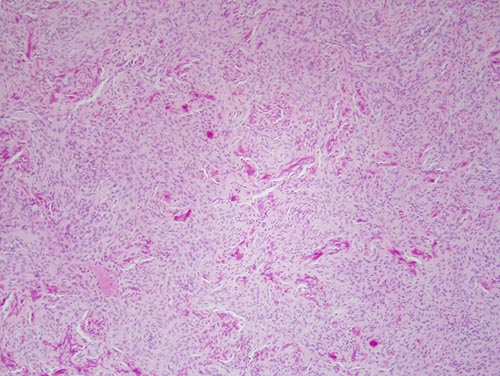
Figure 2. Low power (x100) H & E histology shows a benign fibro-osseous lesions made up of short strands of spindle-shaped fibroblasts focally forming bone. The latter is arranged in clusters of feathery bone in most parts with areas of trabecular bone formation and cementum like material as well as small clusters of giant cells (not shown).
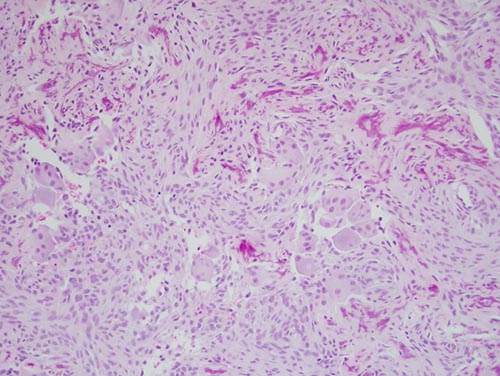
Figure 3. Higher power (x200) H & E histology shows small clusters of giant cells suspended on the cellular connective tissue stroma.
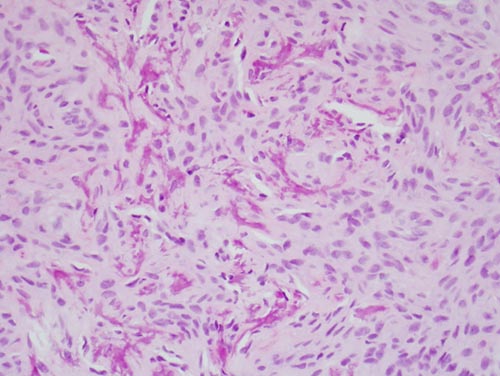
Figure 4. Higher power (x200) H & E histology shows strands of spindle shaped cells suspended on delicate collagen background with clusters of feathery early bone formation.
After you have finished reviewing the available diagnostic information