Irregular radiolucency apical to tooth # 31
Can you make the correct diagnosis?
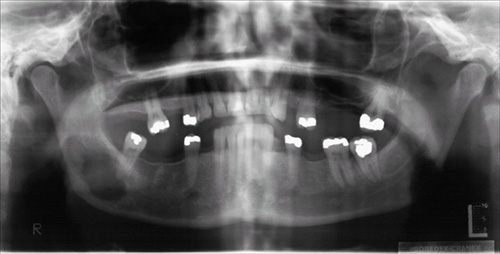
This is a 39-year-old white female who present in September 2006 to the Oral surgery clinic at the University of Washington complaining of pain in her lower right jaw. The patient reported feeling pain in this area in early June 2006. That was followed by tooth #31 gradually becoming loose. The tooth was extracted and the area was biopsied.
Sorry! you are incorrect
Although the associate tooth # 31 shows no evidence of extensive caries to warrant a clinical diagnosis of periapical cyst, the diagnosis nonetheless was entertained because of its apical position and perhaps pulpal death may be the result of trauma which in this case was denied. Periapical cyst is the most common inflammatory or developmental cyst of tooth origin. The tooth is usually necrotic and the etiology is infection due to the non-vital tooth. The inflammation is usually at the apex of the tooth but can be lateral and apical to the tooth. The latter would follow an accessory canal from the side of the tooth. The inflammatory process widens the PDL at the apical part of the tooth and alters the area around the apex. The associated tooth is non-vital, badly carious, fractured or severely periodontally affected. The main etiology is bad caries involving the root canal. The cyst is histologically made up of a lining epithelium, usually non-keratinized stratified squamous epithelium but can also be combined stratified squamous and respiratory epithelium (the latter common in cyst from the maxilla). The epithelial lining is believed to be of remnants of odontogenic epithelium in the vicinity such as the epithelial rests of Malassez. The connective tissue or granulation tissue wall is believed to be the connective tissue reaction to infection from the necrotic pulp. The difference between a periapical granuloma and cyst is mostly in the histologic findings i.e. the cyst would have an epithelial lining while the granuloma would not. Clinically and radiographically, there may not be a difference between the two. Although larger periapical lesions tend to be more in favor of cysts than granulomas, the smaller ones are difficult to differentiate. Radiographically both periapical cysts and granulomas are completely radiolucent and show evidence of widening of the periodontal ligament at the apical or apical lateral aspect of the tooth. Clinical presentation ranges from asymptomatic to painful at percussion. Lesions with abscess and no sinus tract are painful while those with a path to drain are asymptomatic. Swelling is also related to the size of the lesion and the presence and absence of an abscess. Treatment includes endodontic treatment if the tooth is restorable to extraction and curettage of the area. Neither the histology nor the clinical and radiographic findings are in support of a periapical cyst.
Sorry! you are incorrect
Intra-osseous primary malignant neoplasms are rare in the jaw bones. Primary peripheral blood malignant neoplasms such as non-Hodgkin’s lymphoma (NHL) and multiple myeloma (MM) are described in the jaw bones and can present with destructive radiolucencies and ill-defined borders. Around 61% of NHL present extranodally including some in the jaw bones although rarely. The African type Burkitt’s lymphoma is common in the jaw bones but tends to occur in children around 7 years of age. Most of the jaw NHL are of B-cell origin (1-2).
Multiple myeloma is an uncommon malignant neoplasm of plasma cell origin; it can be multicentric arising in several regions at the same time (thus multiple myeloma) or localized (plasmacytoma). Multiple myeloma is characterized by widespread osteolytic bone lesions—especially bones with red marrow such as the skull, ribs, pelvis and mandible (3). This lesion is a disease of patients over 40 years of age, and has a male predominance. Patients usually present with pain, bone fracture, or vertebral collapse. In addition, oral lesions such as amyloidosis are also described. Radiographically, both NHL and MM present in destructive punched out (especially MM) and irregular radiolucencies and moth eaten type of radiolucency. Histologically, both MM and NHL are distinct entities that can be diagnosed and distinguished from each other with the help of a number of histologic markers. The histology of this case was not supportive of either NHL or MM.
Sorry! you are incorrect
It presents as a solitary osseous lesion that can occur anywhere in the body, including the jaw bones, especially that of the posterior mandible. The patient may present with dull pain and tenderness or may be asymptomatic. Patients also may show features of localized severe periodontitis. This condition usually affects younger patients especially children (4-5). Radiographically, it ranges from a well-demarcated but not corticated radiolucency to irregular and destructive radiolucency resulting in teeth “floating in space” type of radiographic morphology. Histologically, it is made up of sheets of Langerhans cells with eosinophils overlying a background of loose and vascular granulation tissue (4-5). Although radiographically this lesion can be an eosinophilic granuloma, histologically it is not.
Congratulations! You are correct
Given the patient’s history of cervical cancer, tumor metastasis has to be considered very seriously in this case. Cancer metastasis to the oral cavity is neither specific nor common. Although it constitutes less than 1% of all oral malignant neoplasms, it may have a devastating result to the patient mainly because metastasis to other sites has already developed or is inevitable (6-7). Theoretically, any malignant neoplasm can metastasize to the oral cavity, but in actuality few do and out of the ones that do, the majority are carcinomas rather than sarcomas. The most common malignant neoplasms that metastasize to the mouth are from the breast, lung, kidney and prostate (6-7). Malignant neoplasms from the thyroid, pancreas, colon, and liver have also been described. Breast cancer is the most common neoplasm to metastasize to the oral cavity regardless of gender. Lung and prostate cancers are the most common neoplasms to metastasize to the oral cavity in men. In most cases, the oral presentation is a secondary diagnosis where the primary diagnosis of the distant organ has been already made and the patient has had or is undergoing treatment for it. This is the case in this case where cervical cancer diagnosis was rendered in February and was treated in March and April. Cervical cancer metastasis to the jaw is extremely rare (8). In fact this may be the second reported case since 1972. Although rare, it is known that on occasion, the oral lesion is the first manifestation of the disease. By far the most common location is the posterior mandible, where 80% of cases occur, followed by the gingiva. The maxilla is a rare location for tumor metastasis. It is mostly described in adults over the age of 30 and rarely in children. Pain and swelling are the most common clinical symptoms, which was the case with this patient. They may also present as asymptomatic, simulating a periapical lesion, gingival swelling like a pyogenic granuloma or it can cause anesthesia and parasthesia, especially when it involves the inferior alveolar canal. The latter results in so-called “numb-chin syndrome.” Tooth loosening, displacement and sharp resorption have also been described and was the case in this patient of 3+ mobility of tooth # 31 associated with pain. The radiographic appearance of irregular bordered unilocular radiolucency is common for metastatic neoplasms to the mandible. The majority of neoplasms cause bony destruction with ill-defined borders, the moth-eaten appearance of some bony destruction indicating aggressive behavior. It is also important to mention that at times, well-demarcated lesions with a benign morphology, as well as cystic radiographic morphology, have also been described. Metastatic neoplasms from the prostate may also be bone-forming, resulting in a radiopaque of mixed radiolucent and radiopaque lesion misdiagnosed as a benign fibro-osseous lesion. As in this case, the diagnosis of tumor metastasis to the oral cavity carries a poor prognosis because the oral cavity is usually not an isolated site and tends to project more disseminated clinical behavior (6-7). Patients are typically treated with chemotherapy and the five-year survival rate is very low.
Treatment
Under local anesthesia, tooth # 31 was extracted and the soft tissue in the area was biopsied. An incisional biopsy was performed of the central mass and peripheral gingiva. The biopsy was predominantly soft tissue with some bony fragments. The area was stabilized with Ivy loops and intermaxillary fixation. The bone was paper-thin especially at the buccal cortex around the angle of the mandible and anteriorly around the body of the mandible. The soft tissue lesion was friable, bled easily, and did not hold sutures. The specimens were submitted for microscopic examination.
References
- Someya M, Sakata K et al. Three cases of diffuse B-cell lymphoma of the mandible treated with radiotherapy and chemotherapy. Radiat Med. 2005; 23: 296-302.
- Rosado MF, Morgensztern D et al. Primary diffuse large cell lymphoma of the mandible. Leuk Lymphoma. 2004; 45: 1049-1053.
- Baykul T, Aydin U et al. Inusual combination of presenting features in multiple myeloma. Dentomaxillofac Radiol. 2004; 33: 413-419.
- Shordone L, Guidetti F et al Langerhans’ cell histiocytosis: a case report of an eosinophilic granuloma of the mandible treated with bone graft surgery and endosseous titanium implants. Int J Oral Maxillofac Implants. 2006; 21:124-130.
- Ardekian L, Peled M, et al. clinical and radiographic features of eosinophilic granuloma in the jaws: review of 41 lesions treated by surgery and low-dose radiotherapy. Oral Surg. Oral Med. Oral Path. Oral Radiol Endod. 1999; 87: 238-242.
- A. Hirshberg and A. Buchner, Metastatic tumours to the oral region. An overview. Oral Oncol. 1995; 31: 355–360.
- Ivan der Waal, RIF, Buter, J. Oral metastases: report of 24 cases. Br J Oral Maxillofac Surg. 2003; 41: 3-6.
- Uhler IV, Fahs GR, Dolan LA. Metastasis of cervical carcinoma to the mandible: report of a case. J Am Dent. Assoc. 1972; 85: 363-364.