Single Purplish-Red, Right Anterior Buccal Gingiva & Maxillary Vestibule
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by: Dr. Galia Leonard
Oral & Maxillofacial Surgery, Seattle, WA
Case Summary and Diagnostic Information

This 12-year-old white female was referred to the oral surgeon in October 2011 for the evaluation of a purplish-red and smooth surfaced nodule in the anterior maxillary vestibule.
Diagnostic Information Available
This 12-year-old white female was referred to the oral surgeon in October 2011 for the evaluation of a purplish-red and smooth surfaced nodule in the anterior maxillary vestibule (Figure 1). This growth is of three to four week duration. It was an isolated and symptomatic lesion and the associated teeth are vital. The area is radiographically normal with no bone resorption.
Figure 1. This photograph was taken at first presentation where a small, dome shaped and smooth surfaced, purplish-red swelling is identified buccal to tooth #6.
The patient’s past medical history is unremarkable.
This was an isolated lesion slowly growing over a three to four week period.
Figure 1. This photograph was taken at first presentation where a small, dome shaped and smooth surfaced, purplish-red swelling is identified buccal to tooth #6.
Treatment
The lesion was completely excised under local anesthesia.
Excisional Biopsy
Histologic examination reveals a hemisected piece of soft tissue composed of thin and keratinized surface epithelium with underlying fibrous connective tissue almost all occupied by loose and vascular granulation tissue (Figure 2). The granulation tissue contains sheets of large “histiocytes” interspersed with multinucleated giant cells and significant aggregates of eosinophils (Figure 3). The granulation tissue is also infiltrated by many plasma cells, lymphocytes and neutrophils. Using Immunohistochemistry staining, the “histiocytes” were uniformly positive with antibody to CD1a (Figure 4).
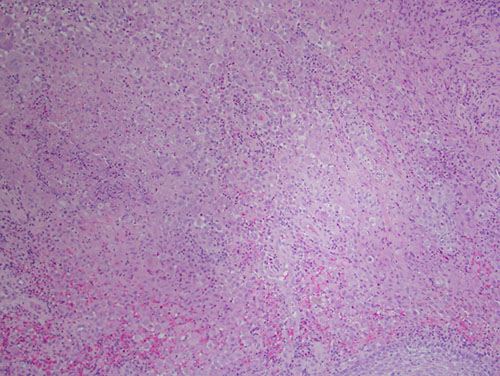
Figure 2. Low power (x40) H & E stained histology shows a mass of vascular granulation tissue containing sheets of large “histiocytes” interspersed with multinucleated giant cells and significant aggregates of eosinophils.
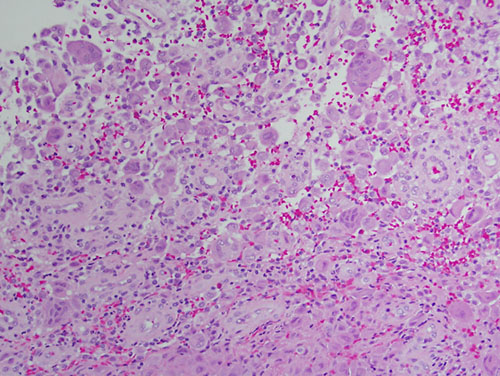
Figure 3. Higher power (x200) H & E stained histology shows a mass of vascular granulation tissue containing sheets of large “histiocytes” interspersed with multinucleated giant cells and significant aggregates of eosinophils.
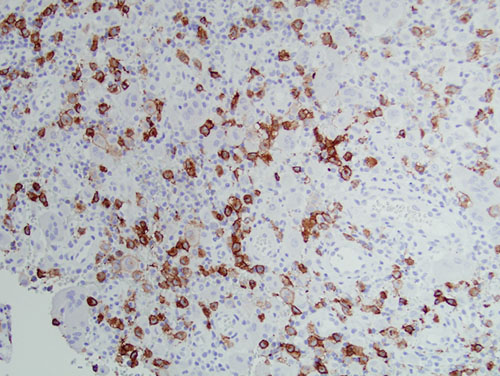
Figure 4. High power (x200) Immunohistochemistry stain with antibody to CD1a, the “histiocytes” were uniformly positive with this antibody.
After you have finished reviewing the available diagnostic information