Return to Case of the Month Archives
August 2009: Swelling right posterior hard palate
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Adam Fettig
Oral & Maxillofacial Surgery, Kirkland, WA
Case Summary and Diagnostic Information

This is a 58-year-old white female with a small and slightly raised swelling on the posterior hard palate of two months’ duration (Figure 1). The swelling is asymptomatic and is soft in consistency with an intact mucosa; it is 1 x 1 cm at its greatest dimensions. It is pink to focally light blue. This patient has palatal torus that has been present for many years; this lesion is to the right of the palatal torus.
Diagnostic Information Available
This is a 58-year-old white female with a small and slightly raised swelling on the posterior hard palate of two months’ duration (Figure 1). The swelling is asymptomatic and is soft in consistency with an intact mucosa; it is 1 x 1 cm at its greatest dimensions. It is pink to focally light blue. This patient has palatal torus that has been present for many years; this lesion is to the right of the palatal torus.
Figure 1 This photograph was taken at the first clinical presentation; note the swelling on the right and lateral posterior hard palate; right of the torus palatinus. The swelling is focally light blue in color and the overlying mucosa is intact.
The patient’s past medical history is significant for smoking for ten years, appendicitis and appendectomy.
The patient reported a slowly enlarging lesion in the posterior hard palate of approximately two months’ duration. The swelling was not painful and was pink to focally light blue in color. This patient has torus palatinus in the mid-posterior hard palate while the lesion is to the right of the torus palatinus.
Treatment
Under local anesthesia, an incisional biopsy was performed. Based on the biopsy results, the patient was referred to an ENT surgeon for complete surgical removal with clean margins. Under general anesthesia, the lesion was completely excised and the area healed with a 2mm small nasal fistula but no nasal regurgitation. Healing was slow and antibiotics and pain medications were prescribed post-operatively.
Incisional Biopsy
Histologic examination of the H & E section revealed a piece of soft tissue made up of a neoplasm of salivary gland origin covered by stratified squamous epithelium and surrounded by minor salivary gland tissue (Figure 2). The neoplasm is infiltrative and is made up of mucous-producing cells surrounded by epidermoid cells. The neoplasm is arranged in a duct-like structure with some cystic degeneration. The mucous-producing cells comprise the bulk of the specimen while the epidermoid cells constitute a smaller portion and are mostly at the periphery of the cystic and duct-like structures lining the mucous producing cells (Figure 3). The neoplastic cells are suspended on mature connective tissue stroma.
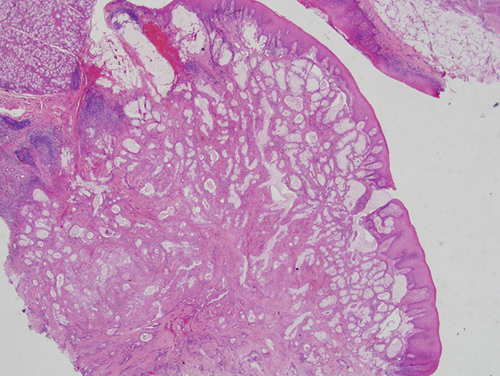
Figure 2 Low power (x40) H & E histology demonstrates duct-like structures with focal cystic degeneration. These structures are lined by layers of mucous producing cells and epidermoid cells. The latter are at the periphery while the mucous producing cells are present intraluminally.
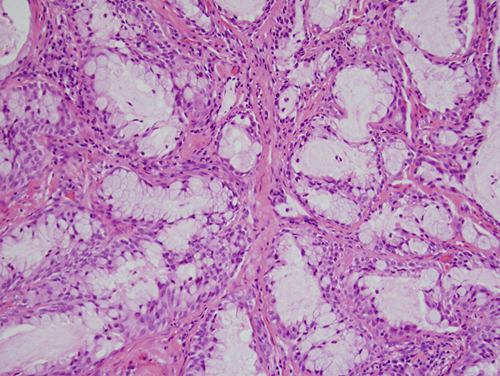
Figure 3 Higher power (x200) H & E histology demonstrates closer look at the duct-like structures with mucous producing cells and epidermoid cells at the periphery.
After you have finished reviewing the available diagnostic information