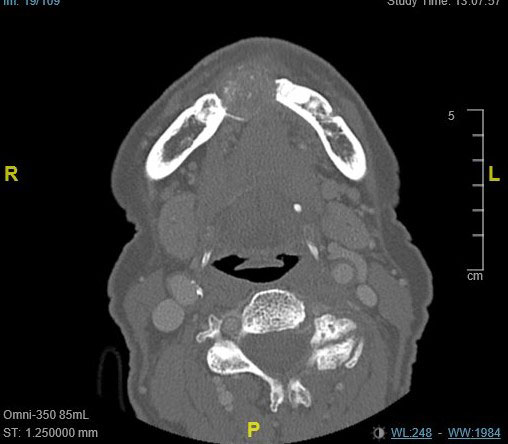
April 2021: Large & expansile mixed radiolucent/radiopaque mass: Right mandible
Can you make the correct diagnosis?
This is an 89-year-old female whose chief complaint is that her dentures are not fitting on the right side of her lower jaw.
Sorry, you are incorrect!
The lesion’s site in the posterior mandible, expansion, and mixed radiolucency and radiopacity, combined with the patient’s gender, are all features consistent with the clinical and radiographic behavior of central odontogenic fibroma. The well-demarcated lesion is also consistent with central odontogenic fibroma. This patient’s age is not consistent with this condition, however; it is beyond the high end of the age range, which is typically 80 years of age. The histology is not consistent with central odontogenic fibroma.
Central odontogenic fibroma is a rare neoplasm of mesenchymal odontogenic origin. Histologically, it is made up of connective tissue stroma with odontogenic epithelial nests and may or may not have calcified material simulating cementum globules. Central odontogenic fibroma occurs in a wide age range of 9-80 with a mean patient age of 40 years. It occurs more commonly in females with a ratio of 2:1 or 7:1, depending on the studies reported. About 60% of cases occur in the anterior maxilla and the rest in the posterior mandible, usually between teeth, though about one third are associated with impacted teeth. Some of the neoplasms that occur in the maxilla can cause palatal depression (dimpling) of the hard palate below where the neoplasm is. These neoplasms are slow growing but can reach large sizes. They can resorb and displace teeth as well as cause tooth mobility. Radiographically, they can be unilocular or multilocular, expansile, and completely radiolucent. In about 12% of cases, they can be radiolucent with flecks of radiopacity.
Sorry, you are incorrect!
The site of this case makes a diagnosis of CGCG more likely; it is anterior to the first molar, and 70% of CGCG cases occur in the mandible anterior to the first molar. The mixed radiolucent/radiopaque radiographic presentation is not typical for this condition because the majority of cases present as multinodular and radiolucent in presentation. In addition, the age of this patient is not typical of CGCG since about 60% of cases occur in patients under the age of 30. The gender of this patient is consistent with CGCG since this lesion affects females more often than males with a female-to-male ratio of 2:1. CGCG can, at times, produce bone and that can account for the mixed RL/RO radiographic findings. The histology, however, is not consistent with CGCG.
CGCG is a non-neoplastic condition that occurs in patients younger than 30 years of age about 60% of the time, typically in the mandible. It is twice as common in females as in males. Over 70% of cases occur in the mandible anterior to the first molar tooth. The other 30% occur in the maxilla. CGCG can be surgically removed or treated alternatively. The alternative treatment of CGCG includes local steroid injections or calcitonin spray to inhibit the osteoclastic activity. Also used are subcutaneous injections of interferon-alpha which have an anti-angiogenic effect. Intravenous bisphosphonates have been used to treat CGCG with some success.
Sorry, you are incorrect!
The multilocular and expansile lesion, when combined with the gender of this patient, could indicate primary hyperparathyroidism. The age is on the older side of the typical age range but can also be suggestive of this condition. The presence of the radiopaque spots is not typical of hyperparathyroidism, but bone can be present between the soft tissue components. The histology, however, is not consistent with hyperparathyroidism.
Hyperparathyroidism is the result of excessive production of parathyroid hormone (PTH) needed for calcium release. PTH stimulates the osteoclasts to resorb bone and release calcium unto the blood stream. When too much PTH is present, there will be generalized bone resorption but more so in the small bones such as the jaws and the small finger bones. There are two types of hyperparathyroidism: primary and secondary; primary is the type that applies to this case. Primary hyperparathyroidism is associated with parathyroid adenoma, but possibly parathyroid hyperplasia and rarely adenocarcinoma. Secondary is usually associated with chronic renal disease (renal osteodystrophy) where ions such as calcium are lost through renal failure and demand for calcium production comes as a secondary factor. This patient has normal kidney functions.
Primary hyperparathyroidism is three times more common in females than in males; it is especially common in females in their fifties and sixties. It may produce multiple bone lesions known as ‘brown tumor’ because of the chocolate color of the soft tissue within the bone. “Stones, bones, moans and groans” are clinical characteristics associated with this condition. Laboratory tests show increased levels of PTH. Hypercalcemia may be present which may be accompanied by hypophosphatemia. Radiographically is associated with loss of density which can range from irregular radiolucent lesions that may be multiple or may have a ‘ground-glass’ appearance which is close to the radiographic changes in this patient.
Sorry, you are incorrect!
The patient’s age argues against this lesion since it is more than twice the typical average age of 35 years. The site and buccal and lingual expansion of the posterior premolar area of the mandible, however, is consistent with COF. The mixed radiolucent and radiopaque changes are also consistent with COF.
Central ossifying fibroma is a benign neoplasm of the jaw bones that presents radiographically as a well-demarcated to corticated radiolucent or mixed radiolucent/radiopaque mass with a peripheral radiolucent rim. Central ossifying fibroma is a slow-growing, expansile lesion with characteristic downward expansion of the inferior border of the mandible which was not noted in this case. It can also expand buccally and lingually. The associated teeth are vital. It is common in young adults around 35 years of age and is five times more likely to occur in females than males. It affects the posterior mandible in about 90% of cases.
Congratulations, you are correct!
The buccal and lingual expansion and occurrence in the posterior mandible are consistent with the presentation of solid ameloblastoma. The patient’s age, however, is very advanced for this condition and the patient’s gender is not applicable because ameloblastoma occurs equally in males and females. The radiographic presentation of a mixed radiolucent and radiopaque lesion is not typical of conventional ameloblastoma but can indicate desmoplastic ameloblastoma. The histology, however, is not desmoplastic ameloblastoma.
The histology is a combination of odontogenic keratocyst and ameloblastoma that has been characterized by some as a very rare variant of ameloblastoma called keratoameloblastoma.
Keratoameloblastoma is an exceptionally rare condition of odontogenic origin. This entity is histologically characterized by excessive keratin formation and in some cases by production of woven bone in foci throughout the connective tissue. Bone formation seem to be a unique feature associated with this to this entity. The literature is neither uniform or clear on the origin of this condition; some consider it to be a variant of acanthomatous ameloblastoma while others suggest it is a solid and confluent form of odontogenic keratocyst. There are far too few cases of this entity to form a conclusive opinion or project a clinical and behavioral profile. But generally speaking solid ameloblastoma are benign but locally aggressive neoplasms that have a high recurrence rate.