Large & Completely Asymptomatic Swelling of the Posterior Tongue
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by Dr. Namou Kim
Director Head & Neck Surgery, Swedish Medical Center, Seattle, WA
Case Summary and Diagnostic Information

This is a 58-year-old male who was completely unaware of a large swelling in the posterior tongue.
Diagnostic Information Available
This is a 58-year-old male who was completely unaware of a large swelling in the posterior tongue (Figure 1). The swelling was of unknown duration. It was soft in consistency and was well demarcated per radiographic imaging (Figure 2). The patient’s dentist noticed the swelling and recommended that it be evaluated.
Figure 1. This is a clinical photograph as the patient first presented to the Swedish Hospital. Note the large, smooth surfaced and deep swelling in the posterior tongue.

Figure 2. This is a CT scan in soft tissue window image demonstrating a well circumscribed soft tissue lesion in the posterior tongue.
The patient’s past medical history is significant for hypertension, hyperlipidemia, eczema and glaucoma.
This swelling was not apparent to the patient but was noticed by the dentist. It was a large soft tissue lesion in the posterior tongue (Figure 1). The CT scan in soft tissue window showed a well-circumscribed soft tissue lesion in the posterior tongue (Figure 2) which measured 3.0 x 2.1 x 3.2 cm.
Figure 1. This is a clinical photograph as the patient first presented to the Swedish Hospital. Note the large, smooth surfaced and deep swelling in the posterior tongue.
Figure 2. This is a CT scan in soft tissue window image demonstrating a well circumscribed soft tissue lesion in the posterior tongue.
Treatment
Under general anesthesia an incision was made through the posterior tongue to release a circumscribed yellow nodule (Figure 3). The soft tissue nodule was bluntly and circumferentially enucleated. It shelled out intact as an encapsulated yellow nodule (Figure 4) of about 3.5 cm in greatest dimensions. The nodule was soft, and upon sectioning it was yellow and glistening. The surgical site was closed with Vicryl suture. The area healed well.
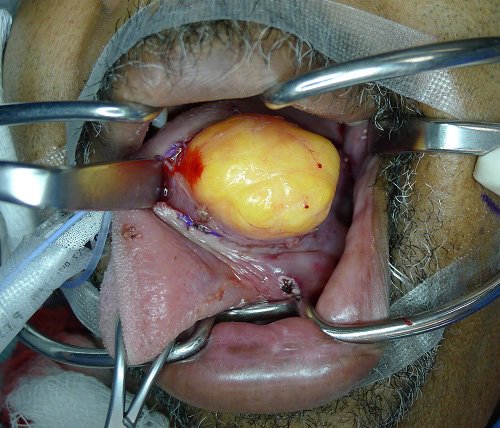
Figure 3. This is a clinical photograph of the lesion at surgery demonstrating a yellow nodule emerging from the site of incision.

Figure 4. This is a gross photograph of the encapsulated yellow nodule after it was removed from the posterior tongue.
Excisional Biopsy
The histology was diagnosed by Dr. Diane Jordan, Cellnetix Pathology, Seattle, WA. Histologic evaluation revealed a multisected and encapsulated neoplasm composed of lobules of mature adipocytes suspended on delicate collagen fibers and small blood vessels (Figure 5 & 6). The neoplasm is surrounded by a thin capsule made up of a few layers of fibrous connective tissue.
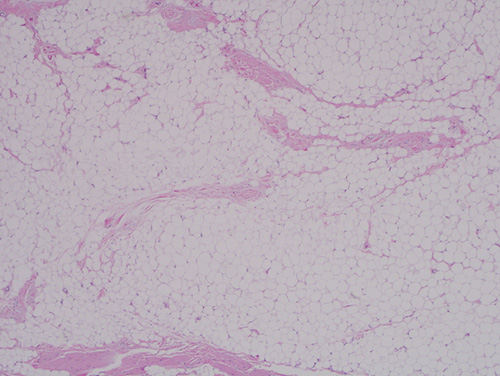
Figure 5. Low power (x100) H & E stained histology shows a benign neoplasm of adipose tissue origin. It is lobular and composed of mature adipocytes suspended on delicate collagen fibers. The adipose tissue is focally infiltrating skeletal muscle bundles.
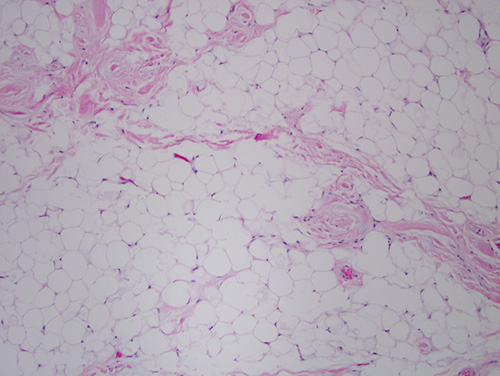
Figure 6. High power (x200) H & E stained histology shows a closer look at the mature adipocytes suspended on a delicate background of connective tissue.
After you have finished reviewing the available diagnostic information