Well Demarcated Mixed Radiolucent/Radiopaque Mass, Right Posterior Maxilla
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Dr. Tracy Johnson
Oral & Maxillofacial Surgery, Lakewood, WA
Case Summary and Diagnostic Information

This is a 30-year-old female who self-referred for wisdom tooth removal. The oral surgeon noted a swelling in the right posterior maxilla of unknown duration which was confirmed by a panoramic radiograph.
Diagnostic Information Available
This is a 30-year-old female who self-referred for wisdom tooth removal. The oral surgeon noted a swelling in the right posterior maxilla of unknown duration which was confirmed by a panoramic radiograph. The radiograph shows a well-demarcated mixed radiolucent/radiopaque lesion between teeth #s 3 and 4 (Figure 1). It is buccally and palatally expansile, pushing superiorly into the right maxillary sinus. It is displacing teeth #s 3 and 4 apart and is described to be 2 x 2 x 1.7 cm in size. It is otherwise asymptomatic and the involved teeth are vital.
Figure 1. Panoramic view at first presentation demonstrating a well demarcated and partially corticated RL/RO lesion between teeth #s 3 and 4. This mass is displacing teeth and is expansile pushing superiorly into the maxillary sinus.
The patient’s past medical history is unremarkable.
A large swelling was identified by the oral surgeon in the right posterior maxilla but was unknown to the patient who self-referred for wisdom tooth removal. The swelling was large and asymptomatic. It was expanding bone buccaly, palatally and superiorly into the right maxillary sinus. It was pushing teeth #s 3 and 4 apart and the teeth were vital. The swelling was described to be 2 x 2 x 1.7 cm in size.
Treatment
Under IV sedation, the area was surgically exposed where the overlying bone was found to be very thin (Figure 2). The bone was removed and the lesion exposed (Figure 3). The area was curetted, irrigated and closed. There was a small perforation through the maxillary sinus but that healed along with the rest of the area without any complications.
Excisional Biopsy
Histologic examination reveals multiple and multisected pieces of soft tissue embedded in five separate blocks. All specimens showed evidence of a neoplasm made up of myxoid connective tissue containing calcified material (Figures 4-6). The connective tissue comprised the bulk of the specimen and was loose and vascular and was made up of spindle-shaped cells that were positive with smooth muscle actin but negative with S-100. Some of the finbroblasts were forming whorls. The calcified material was cementum-like. Occasional odontogenic epithelial islands were identified.

Figure 2. This photograph is taken during surgery partially exposing the encapsulated lesion with intact thin bone covering the lesion.
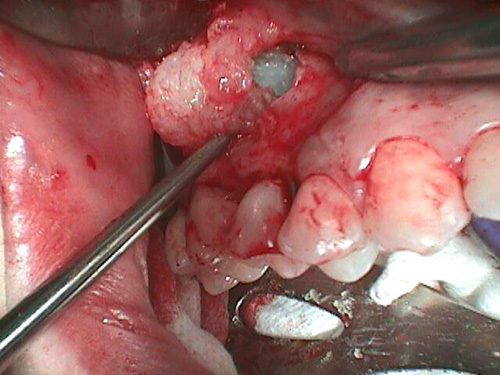
Figure 3. This photograph is taken during surgery with some bone removed and the myxoid looking lesion partially exposed and in the process of being curetted.
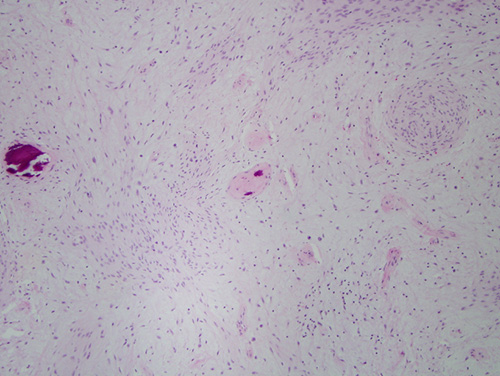
Figure 4. Low power (x40) H & E histology shows myxoid connective tissue with focal spindle-cell whorling and cementum-like calcifications.
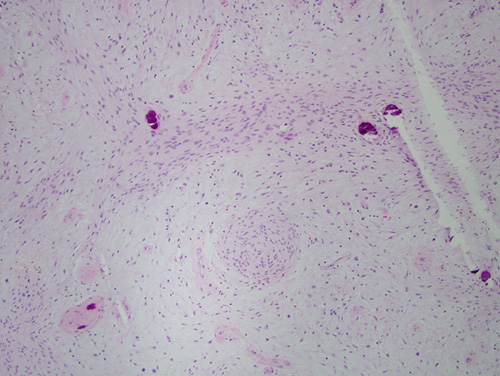
Figure 5. High power (x100) H & E histology with closer look of the myxoid connective tissue, spindle-cell whorling and cementum-like calcified material.
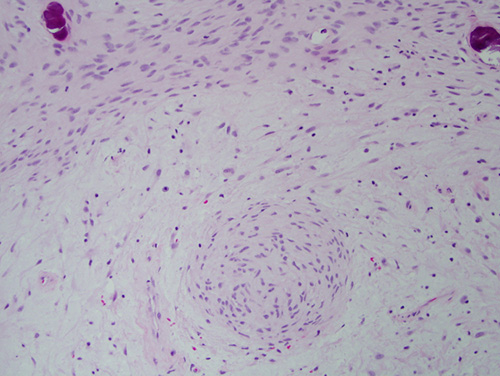
Figure 6. High power (x200) H & E histology with even closer look of the myxoid connective tissue, spindle-cell whorling and cementum-like calcified material.
After you have finished reviewing the available diagnostic information