Return to Case of the Month Archives
Maxillary gingival and palatal swellings
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. Pardeep Brar, Ryan Gibson, Ross Beirne
University of Washington, Seattle, WA
Case Summary and Diagnostic Information

This is a 44-year-old African-American male who first presented to his physician for a skin problem and scaling of the scalp. The skin problem was diagnosed as psoriasiform dermatitis and was treated with desonide 0.05% ointment twice a day. For the scalp scaling, he was using ketoconazole 2% and selenium sulfide shampoos on a regular basis.
Diagnostic Information Available
This is a 44-year-old African-American male who first presented to his physician for a skin problem and scaling of the scalp. The skin problem was diagnosed as psoriasiform dermatitis and was treated with desonide 0.05% ointment twice a day. For the scalp scaling, he was using ketoconazole 2% and selenium sulfide shampoos on a regular basis. On one of his clinical presentations to his dermatologist, he complained about three enlarging nodules in his mouth: one on the anterior hard palate, one on the soft palate and a third enlarging purplish-red swelling on the maxillary buccal gingiva between teeth #s 5 and 6 (Fig 1). He was referred to Dr. Beirne for evaluation of the swellings. He stated that these lesions were not painful but that they were growing fast and were bothersome. The soft palate lesion was obstructive to the oropharynx.
The patient’s medical history is significant, as he is HIV positive. He has no drug allergies. In January 2006, he was admitted to the Harborview Medical Center with pneumonia. He was immunocompromised and has recently been placed on antiretroviral medications. In addition, he has nodular skin rash and seborrheic dermatitis.
Three large purplish-red exophytic lesions were identified: one on the maxillary buccal gingiva between teeth #s 5 and 6 (Fig 1), one on the anterior hard palate, and the third on the soft palate (Fig 2). All three lesions were not painful and were highly vascular. The gingival lesion was sessile; the soft palate lesion was pedunculated and was approximately 2.5 cm x 3 cm in size, and the anterior hard palate lesion was also pedunculated. On clinical examination, all three were firm on palpation and bled easily. The lesion on the buccal maxillary gingiva was approximately 6 to 8 mm in size. The lesions on the palate were over a centimeter in size each and, per the patient’s report, had doubled in size in the past two weeks.
Figure 1. Kaposi’s sarcoma presenting as exophytic, sessile, red gingival swelling simulating a pyogenic granuloma. This is an unusual presentation for KS.

Figure 2. Kaposi’s sarcomas involving the soft palate and anterior hard palate. Note the purplish-red color, both are exophytic and the soft palate lesion is obstructive to the oropharynx.
The histologic diagnosis of this biopsy was rendered by the pathologists at Harborview Medical Center, Seattle, WA. The histologic examination reveals a highly cellular and vascular neoplasm arranged in small nodules (Fig 3) in some areas and in a haphazard manner in others. It is made up of interlacing fascicles of monomorphic spindle cells with mild cellular and nuclear atypia (Fig 4). The mitotic activity is noticeable and frequent (Fig 4). These cells are arranged around slit-like vascular spaces, some with erythrocytes. This neoplasm is extensively positive with CD34 (Fig 5) and HHV8 antibodies (Fig 6).
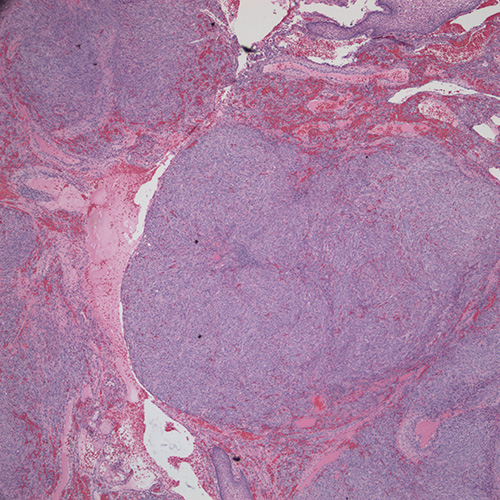
Figure 3. Low power (x20) histology shows a nodular appearance of the neoplasm. This screening magnification clearly demonstrates the high cellularity of this neoplasm.
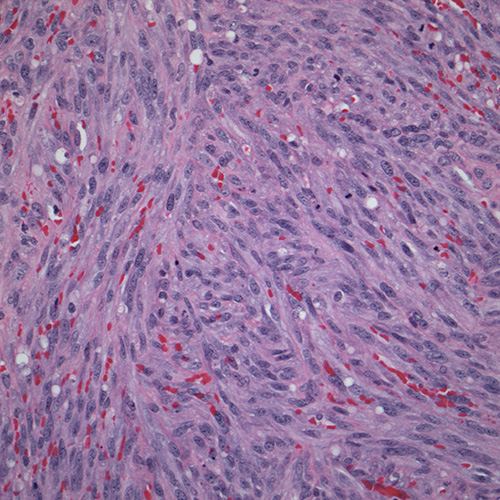
Figure 4. Higher power (x200) histology shows the interlacing fascicles of spindle cell with mild atypia surrounding slit-like arrangement of blood vessels, some with erythrocytes. Note the frequent mitotic activity.
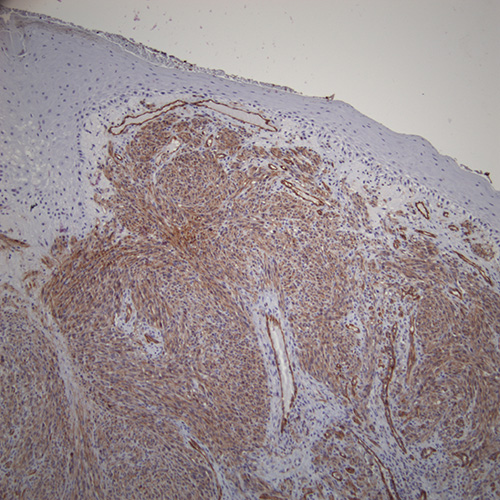
Figure 5. Figure 5 Low power (x100) Immunohistochemistry stain with CD34. Note the strong positive spindle cells components as well as the small blood vessels.
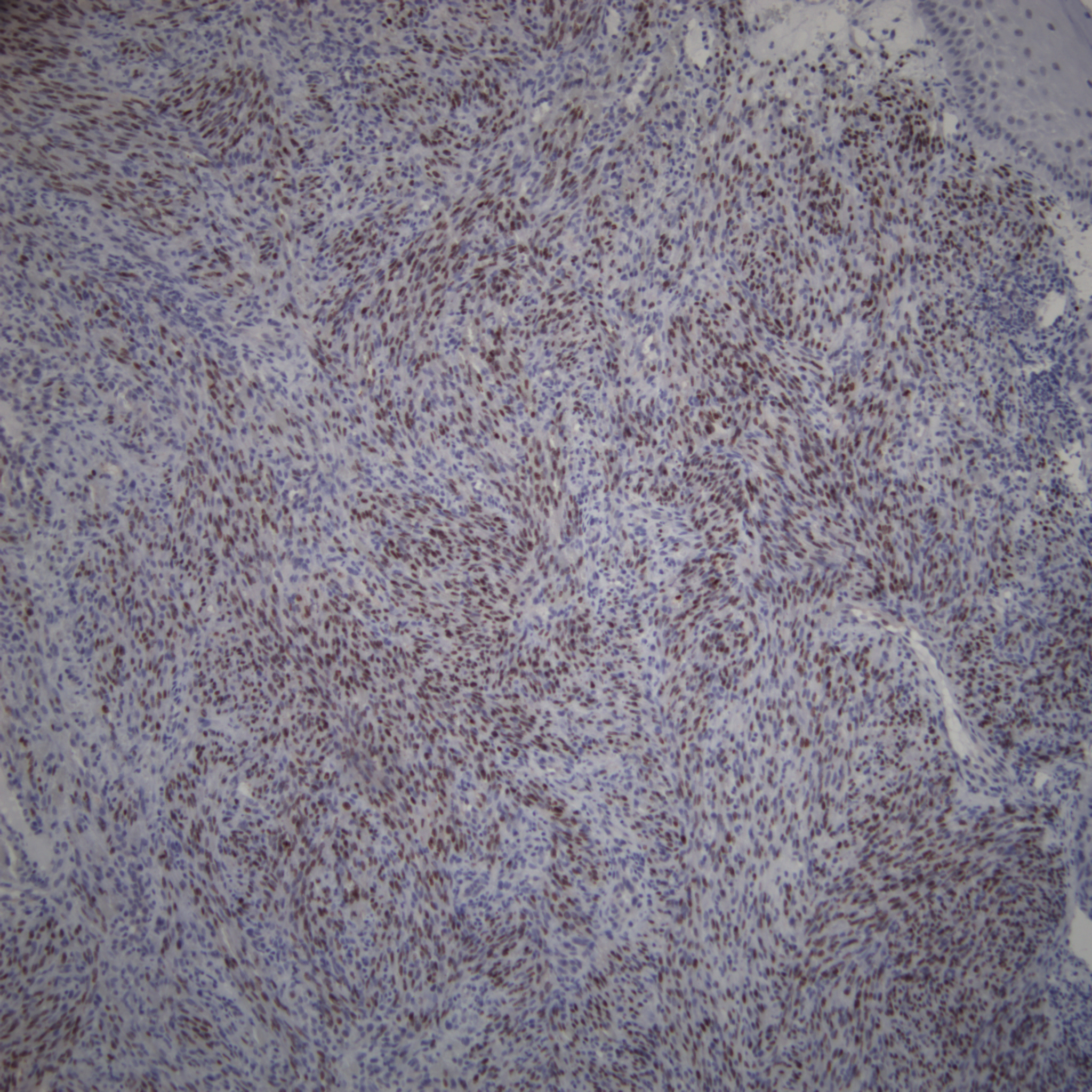
Figure 6. Figure 6 Low power (x100) Immunohistochemistry stain with HHV8. Note the strong positive staining of the tumor cells.
After you have finished reviewing the available diagnostic information