Return to Case of the Month Archives
Large radiolucent/radiopaque lesion right posterior mandible and ramus
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Drs. Todd carter and Barry Shitamoto
Maui Oral & Maxillofacial Surgery & Maui Memorial Medical Center, Maui, HI
Case Summary and Diagnostic Information

This is a 17-year-old Hawaiian male whose chief complaint is of right facial swelling and asymmetry of six months’ duration.
Diagnostic Information Available
This is a 17-year-old Hawaiian male whose chief complaint is of right facial swelling and asymmetry of six months’ duration. The patient has had regular dental and medical care. The patient was originally seen by an ear, nose and throat doctor who attributed the facial asymmetry to a large and expansile radiolucency of the right posterior mandible and ramus (Figure 1); this was confirmed by an oral surgeon. There was no evidence of pain, neurological abnormalities or malocclusion. The condyle and coronoid processes were not affected.
Figure 1 Cone Beam CT view at first presentation demonstrating large unilocular and expansile radiolucency with some generalized fine radiopacity involving most of the right posterior mandible and part of the ramus sparing the condyle and the coronoid processes.
The past medical history is significant for heart murmur and severe aortic coarctation.
The panoramic radiograph demonstrates a large, well-defined and corticated unilocular radiolucent lesion occupying a significant portion of the right posterior mandible and involving part of the right ramus but sparing the condylar and coronoid processes. The lesion was expansile, leading to facial asymmetry.
Figure 1 Cone Beam CT view at first presentation demonstrating large unilocular and expansile radiolucency with some generalized fine radiopacity involving most of the right posterior mandible and part of the ramus sparing the condyle and the coronoid processes.
Treatment
The treatment was delayed for about six months to first care for the severe aortic coarctation, which was stented. The area was treated with extensive enucleation and curettage. Coronoidectomy and extraction of teeth #s 30 & 31 were performed to allow good visualization into the proximal portion of the lesion. If the lesion recurs, the area will be curetted again and the patient placed on interferon therapy.
Incisional Biopsy
The incisional biopsy demonstrated multiple fragments of decalcified hard and soft tissue made up of a benign fibro-osseous lesion (Figures 2 and 3). It is composed of irregularly shaped and woven-type bony trabeculae surrounded by cellular fibrous connective tissue stroma. The bony trabeculae are of variable shapes and sizes; some show significant osteoblastic rimming. In focal areas, the connective tissue stroma has clusters of multinucleated giant cells (Figure 4).
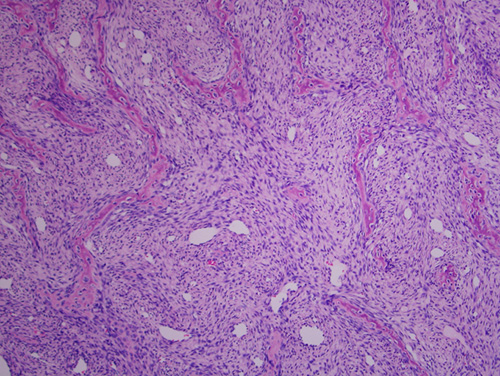
Figure 2 Low scanning power (x40) histology shows a benign fibro-osseous type lesion composed of irregularly shaped and woven-type bony trabeculae surrounded by cellular fibrous connective tissue stroma.
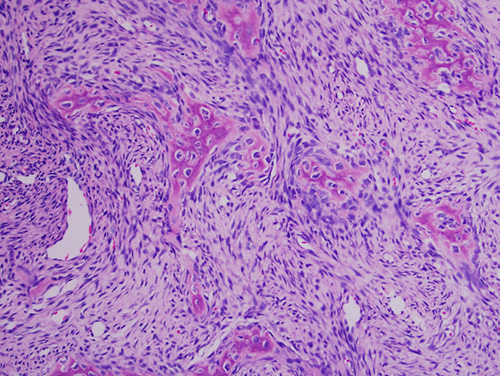
Figure 3 Higher power (x200) histology shows woven bony trabeculae exhibiting significant osteoblastic rimming.
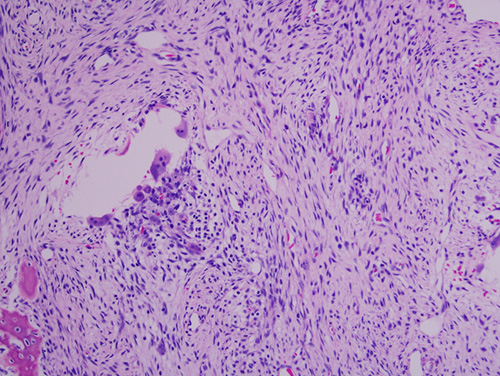
Figure 4 Higher power (x200) histology shows cellular fibrous connective tissue with clusters of multinucleated giant cells.
After you have finished reviewing the available diagnostic information