Return to Case of the Month Archives
Gingival swelling between teeth #s 8 & 9
Dolphine Oda, BDS, MSc
doda@u.washington.edu
Contributed by
Dr. Monty Tolman
Periodontics and Implant clinic, Olympia, WA
Case Summary and Diagnostic Information

This 61-year-old female was referred by her dentist to a periodontogist for evaluation of an enlarging exophytic, slightly lobular, red and ulcerated gingival swelling between teeth #s 8 & 9 (Figure 1). The area was reported to be slightly painful; it was also reported that the lesion was of cosmetic concern to the patient. She is a mouth-breather and had heavy sub-gingival calculus.
Diagnostic Information Available
This 61-year-old female was referred by her dentist to a periodontogist for evaluation of an enlarging exophytic, slightly lobular, red and ulcerated gingival swelling between teeth #s 8 & 9 (Figure 1). The area was reported to be slightly painful; it was also reported that the lesion was of cosmetic concern to the patient. She is a mouth-breather and had heavy sub-gingival calculus.
Figure 1. This photograph was taken at the first periodontology clinical visit. Note the red, lobular gingival swelling between teeth # 8 & 9 and slightly extending to the interproximal area between teeth #s 9 & 10.
The patient’s past medical history is significant for breast cancer surgery in 1991, a cholecystectomy in 1992, hypertension (treated with calcium channel blockers) and fibromyalgia. She denies smoking and reports social alcohol use. She denies any allergies. Her current medications include Celebrex, Singulair, Evista, Levoxyl, Lisinopril/hydrochlorothiazide, Clonazepam and Cymbalta.
The patient presented with a red, ulcerated, lobular gingival swelling (Figure 1) between teeth #s 8 & 9 mostly involving the labial gingiva and extend into the interproximal palatal gingiva (Figure 2). The patient states that over the past several months she noticed her upper incisors separating slightly with irritated gums but no evidence of loose teeth. The clinical examination revealed heavy sub-gingival calculus.
Figure 1. This photograph was taken at the first periodontology clinical visit. Note the red, lobular gingival swelling between teeth # 8 & 9 and slightly extending to the interproximal area between teeth #s 9 & 10.

Figure 2. This photograph demonstrated the interproximal palatal extension of the swelling.
The histology of the incisional and excisional specimens was similar; both showed proliferative epithelium invading the underlying fibrous connective tissue in the form of broad islands and sheets of epithelial cells (Figure 3). The neoplastic epithelial cells showed evidence of loss of maturation, large nuclei with prominent nucleoli, high mitotic activity, individual cell keratinization and keratin pearls (Figure 4).
Treatment
The incisional biopsy was performed under local anesthesia while the surgery was performed under general anesthesia. The anterior maxillary alveolar ridge was surgically excised to involve the anterior four incisors. A previously fashioned dental prosthesis was inserted in the site of the maxillary defect, and the cavity was packed with Xeroform gauze.
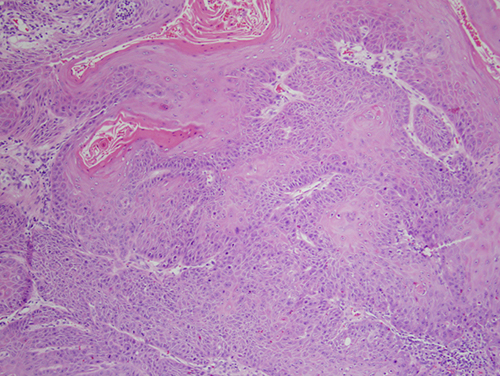
Figure 3. H & E stained section at 100X magnification demonstrating confluent, proliferative, neoplastic epithelial cells cut tangentially.
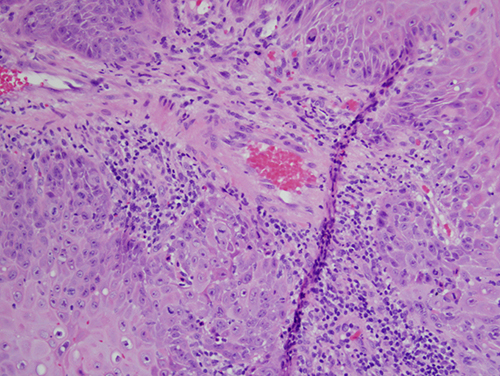
Figure 4. H & E stained section at 200x magnification demonstrating high mitotic activity, large nuclei with prominent nucleoli, nuclear and cellular disorganization, etc, all features of neoplastic epithelial cells.
After you have finished reviewing the available diagnostic information